
What are annual physicals for?
Annual physicals are costly (~$10 billion annually) and have never been shown to improve outcomes, but people value them. In this dichotomy lies a lot of the inner tensions of medical care: between delivery of technical care, and nurturing of human relationships, and those are illuminated by two articles in counterpoint. In the end though both sides come to a point of view that is not altogether dissimilar – that what is needed is not an annual physical, but some sort of preventive care/health review visit which, instead of being a fishing expedition for problems via an assortment of tests, should be a patient-centered exercise to tie up any loose ends of care. Improving Value in Health Care — Against the Annual Physical; Toward Trusting Therapeutic Relationships — In Favor of the Annual Physical (open access)
EHR horror
For many physicians and some patients, the transition to EHRs has been wrenching. A telling vignette quoted by the author of this perspective: “the critical care doctor who, unable to identify new information in daily notes, has begun printing them out and holding two superimposed pages up to the light to see what’s changed.” This is no surprise given for rapid systemic change to occur, it is always imposed from the top or by external constraints, and in these circumstances the pain invariably precedes the gain. But even if it is too early to judge the results of the push for EHRs, there is an obvious lack of customer-centricity in the process – many EHRs feel like a copy paste of an old paper process rather than an attempt to fully leverage a new medium to allow insights into the needs of the patient. Transitional Chaos or Enduring Harm? The EHR and the Disruption of Medicine (open access)
Rationalizing the use of imaging
Advanced imaging (e.g. PET, MRI) is a major source of revenues or costs (depending on the point of view). As a result, CMS has mandated that by 2017, physicians will have to document appropriate use when ordering advanced imaging, something that health systems are looking to implement through Clinical Decision Support (CDS) tools. In this perspective, the authors make an interesting parallel with hospital antibiotic use where the overuse problem is not so much costs, but the development of resistance and where a common approach has been to require the use of certain antibiotics to be subject to approval of the infectious disease (ID) department. In analogy, they propose a local stewardship model for medical imaging to supplement an algorithm based approach. This raises two questions: first the ability of a steward model to consistently ignore the financial incentives of its employer for which medical imaging may be a major source of income. Second, whereas variations in local microbiological ecology justify why a local ID department should be controlling local antibiotic use, it is not evident that this logic carries over to imaging. Medical-Imaging Stewardship in the Accountable Care Era (subscriber access)
Precision medicine comes to prostate cancer
Unlike many other cancers, prostate cancer therapy is not influenced by specific genetic or biochemical characteristics of the tumor. This may be about to change. In a single arm study, 50 patients (49 evaluable) with metastatic hormone-resistant disease who had pretty much exhausted their therapeutic options were given olaparib (Lynparza, Astra Zeneca, approved for ovarian cancer), an agent that leverages DNA repair defects for differential killing of tumor cells. Patients were evaluated for a response, and for mutations affecting DNA repair genes in their tumors. The results were as follow: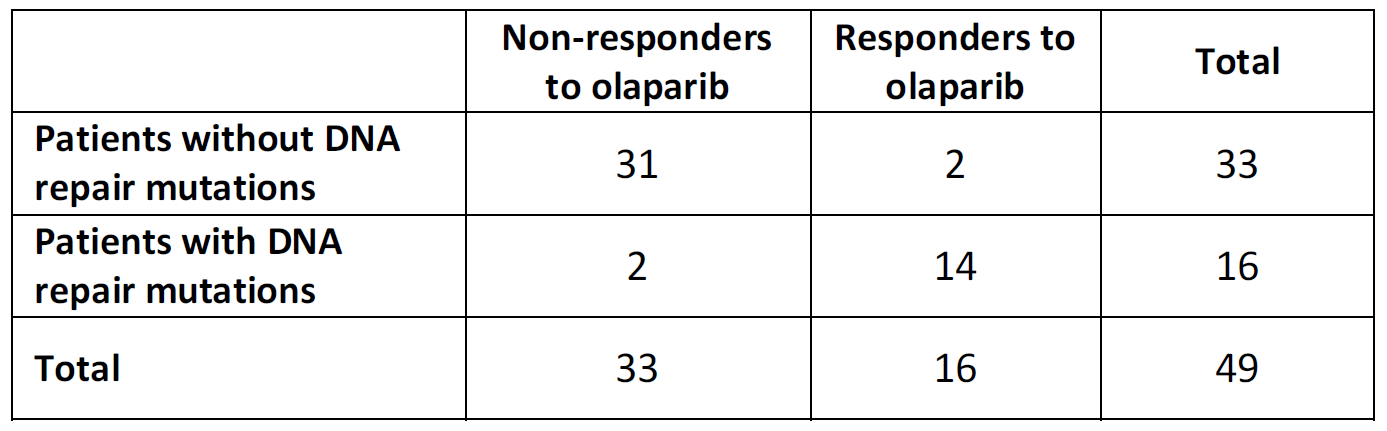
DNA-Repair Defects and Olaparib in Metastatic Prostate Cancer (open access)
Using a melanoma drug for leukemia
Vemurafenib (Zelboraf, Roche) is an approved drug for melanoma when the B-Raf gene has the V600E mutation (which is the case about 50% of the time). Interestingly, the same mutation is a hallmark of the rare hairy-cell leukemia which is usually well managed by classic chemotherapeutic agents. In this study involving the enrollment of 50 patients with hairy-cell leukemia who had relapsed from the usual treatment, 98% (!) had a response to vemurafenib. Consider this another proof point toward development and approval of targeted agents based on biological defect rather than tumor provenance. Targeting Mutant BRAF in Relapsed or Refractory Hairy-Cell Leukemia (subscriber access)
The New England Journal of Medicine is a premier weekly medical journal covering many topics of interest to the health sector. In this monthly series we offer a brief overview of highlights that might be of interest to our clients and others.