
In this morning’s New York Times (June 3,2014), Andrew Ross Sorkin asks,“DO drug companies make drugs, OR money”? That’s a fair question in the context of what I’ll call a “fee-for-product” reimbursement regime. Another way to look at this question is, “CAN drug companies make drugs, AND money”?
Value has not been an easy sell
As the U.S. healthcare services system moves from fee-for-service to a value-based system, the biotech and pharmaceutical (biopharma) industry should have an opportunity to capture more of the value it creates. But with drug costs only ~10% of overall health spending and not growing (thanks to the patent cliff and a slow-down in new blockbusters), payer attention has been on other drivers of cost such as avoidable re-admissions and overuse of emergency rooms. Ironically, this means that while drug companies have been talking up “new business models” that are “value-based” and involve “strategic partnerships with payers”, they’re struggling to get attention in the conference rooms that matter. Of course there are many examples of value-based pricing that the industry can point to but by and large these are limited to specific drugs in specific settings (e.g. Cigna and Rebif) or what I’d broadly classify as disease management or adherence programs. Whatever form these take, they remain a tiny portion of the total biopharma industry.
Uptake has been slow even with Accountable Care Organizations (we use ACOs because these are the most visible of the value based payment methodologies out there today but the basic ideas here apply to any value-based system).
Biopharma expected that drugs would be high on the agenda for ACOs:
- ACOs need to save money and the right medication at the right time saves money through avoided medical treatment.
- ACOs need to meet quality objectives in order to collect their bonuses and medications either directly or indirectly support many of these objectives (in fact over half the metrics in the Medicare Shared Savings Program rely on appropriate use of medications).
But with a few notable exceptions (see this article by Aman Bhandari et al on the Merck/ Heritage challenge), ACOs have not paid particular attention to biopharma business models. Indeed, even the fact that retail drugs are excluded from most ACO
baselines (which in the short term was seen as good for makers of these drugs) has meant that providers have not for the most part needed to consider the economic trade-offs between drugs and medical treatment (that is wehere they may loosely be called substitutes). Also most ACOs have chosen to rely on their respective managed care or PBM formularies simply because they don’t have sufficient scale (yet) to drive purchasing economics.
Not one-size-fits-all
Expanding isolated models of value-based purchasing to the broader drug market requires understanding how multiple factors interact in order to offer up the right model for the right drug. These factors include not only commonly cited characteristics such as the clinical and economic value of each drug but also how different segments of the system evolve relative to these characteristics. Commonly considered factors in determining a value-based model include considering whether a drug:
- is chronic or acute
- prevents future medical costs
- impacts a quality metric (e.g. A1C level) or performance metric (e.g. readmissions)
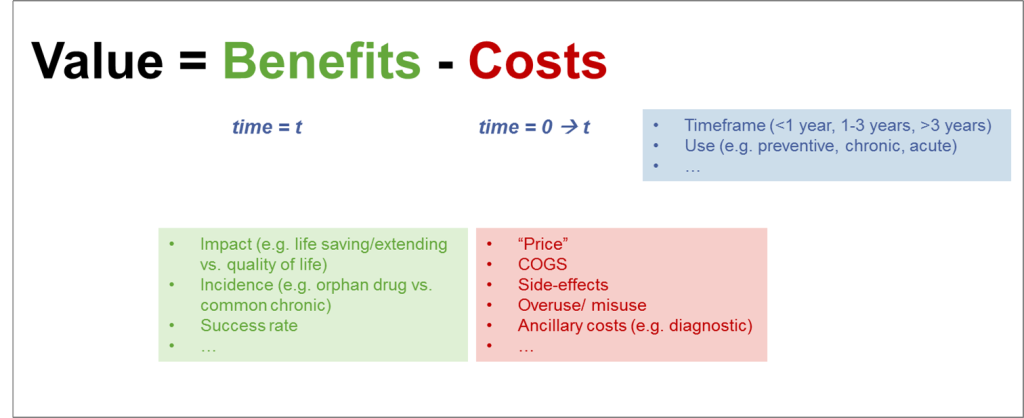
While these are important, there are many additional factors that firms need to consider holistically. We have found it useful to frame these factors using the basic value equation. Note that benefits in general are uncertain and accrue at some future point in time so must be discounted while costs are certain and usually start accruing immediately.
The right model varies depending on how these factors add up for a particular drug. Take just 3 simple examples:
- Consider an expensive drug that delivers a significant clinical impact in a relatively short observable time-frame but does so only for some patients it is indicated for but has no efficacy on others. If it has relatively low COGS and a tolerable side-effect profile, then an appropriate value-based mechanism could be a “guarantee”. For instance J&J reimburses the NHS for patients who do not respond to Velcade.
- Next consider a low-cost drug that treats a symptomless condition in a high incidence condition over a long period of time and that reduces the risk for a future emergency event. Success rate for this treatment is tied to adherence. Here a guarantee is not the right mechanism. An appropriate value-based mechanism could be a payment for services that improve patient engagement and adherence (as a predictor of future medical cost savings). Some of the common chronics and many of the pharma driven DM programs fall into this category.
- Finally, consider an antibiotic that has the potential to be overused or misused leading to antibiotic resistance. Or an opioid pain killer that’s often abused. In each of these cases, the value-based model needs to align the biopharma goal with appropriate antibiotic stewardship and should reward the reduction of overuse or misuse. This is somewhat analogous to the electric utility that has a responsibility to urge customers to reduce consumption of its own product.
ACO segments
It’s not enough to select a revenue model based on value characteristics of the drug alone. Obviously we need to factor in ACO characteristics. One barrier to doing this systematically is the cliché, “If you’ve seen one ACO, you’ve seen one ACO”. Perhaps some truth in it but it’s way overstated. Indeed it is possible to classify ACOs in segments that are relatively homogeneous in terms of how their economics and behavior interact with biopharma value-based models.Others have looked at ACO segments in terms of their ownership and governance but there are additional factors that influence their interaction with manufacturers and vendors such as:
- Scope (what’s in / out) e.g. whether retail drugs are included in their benchmark
- Scale e.g. are they large enough to have their own formulary
- Level of risk: e.g. what % of total revenue is actually at risk
- Risk model: e.g. one-sided or two-sided risk
- Capabilities: e.g. data analytics/ patient engagement…
- Contract time-frame: e.g. value equation is very different for a 1 year contract vs. a 3 year contract
- Quality and performance metrics: e.g. how do drugs affect metrics
So…can they?
Unequivocally yes! The move to value-based models is good for patients and for the health of the nation and for those biopharma firms that play the value game right. The winners will be those who can bring effective drugs to market AND select the right revenue model for the right context.