
In a recent study, Ryan, Shortell, et al analyzed the composition of PCP compensation (broken down into salary, productivity and quality/other components) across practices with ACO contracts vs. those with more traditional business models. This note will:
- provide a quick summary of results
- offer an alternative interpretation of the data
- describe two methodological points regarding the data set
The major finding
As of 2012/2013, there are no major systematic differences in how PCPS are paid in ACO practices vs. others. Whether in an ACO or not, PCPs were paid on average ~50% on salary, ~45% on productivity and 5% on quality/other.
To be sure, in this last, catch-all category, quality (vs. “other”) is much more important piece in ACO participating practices vs. those not participating. Overall, quality’s share of PCP compensation is 2.2 percentage points higher in ACO practices vs. those without an ACO (e.g. quality is 1.5% of total compensation in non-ACO practices, but 3.7% in ACO practices). Statistically significant but “small beer” argue the authors.
They offers two broad hypotheses (with variations) for why ACO practices pay the same:
- “Early days” ACOs are new and practices may not have figured out how they should compensate PCPs optimally; Also, ACO deals are still too small a share of the practice business to disrupt the whole model.
- “All good” The mix (with the little quality kicker) may be appropriate given what ACOs need PCPs to do; also, maybe the real driver of ACO performance isn’t PCP alignment but the quality of the population health infrastructure, nurse care managers, etc.
Compelling hypotheses. Yet they are clearly concerned by the result and ask: “If physicians in ACOs and physicians outside ACOs are paid similarly, will they practice similarly?” They conclude “If incentives are not aligned between practices and physicians, the ACO programs may have limited effects on costs and quality in the short-term.” Uh-oh.
Variety is the spice of life
There are a couple reasons to interpret the results more optimistically.
First, given there was no major difference in compensation strategies among ACO and non-ACO practices (=no selection bias for opting into the program), physicians themselves apparently do not see their compensation systems as barriers to participating in an ACO.
Second, take a look at their Figure 1. In describing the data, the team reveals the startling variety in compensation strategies for PCPs. Eyeballing the chart, there appear to be at least six different segments across the entire data set:
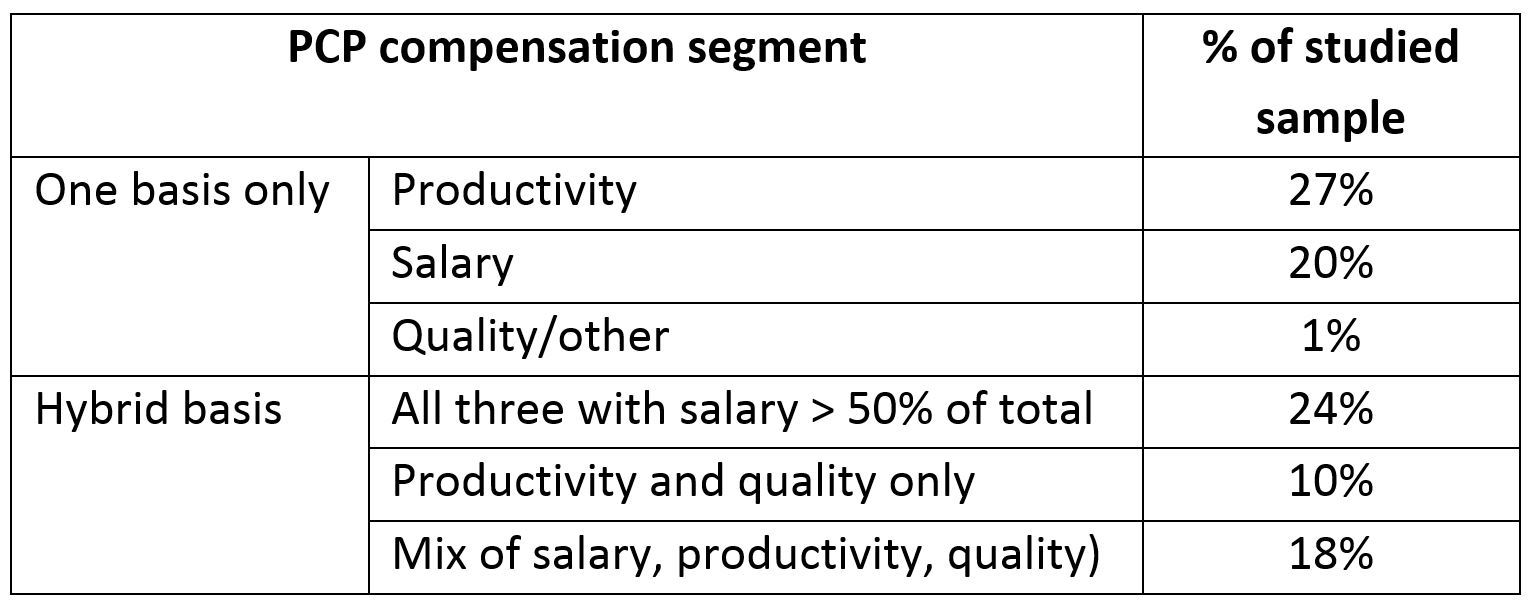
Apparently, despite many decades operating in FFS environment, the market has not discovered one right way to pay PCPs to fit this reimbursement model. Perhaps, therefore, we should not be too worried if there ends up being no one right way to pay PCPs in an ACO. What drives compensation models may have less to do with reimbursement and more to do with practice culture, history, organization structure and operating model (e.g. mix of partners vs. per diem doctors). In fact the team was unable to find many statistically significant drivers of compensation structure (health system ownership vs. physician ownership had some modestly significant impact but most other variables were insignificant. R-squared values were not reported).
Implication? Practices may, in fact, not need to change their compensation structure dramatically to succeed as an ACO in the near-term or otherwise. Given how ugly compensation change discussions can be in physician practices, that would be very good news for the future proliferation of ACOs.
Two methodological points
Two other reasons why the ACO-linked incentives the authors were expecting weren’t evident in the data they studied:
Lack of payout on incentives does not mean the incentives weren’t there. Composition of actual compensation (the question posed by the survey) may simply reflect poor performance vs. potential, not necessarily absence of incentives to deliver on ACO objectives. Just because “quality / other” components made up the same share of PCP compensation across all practices does not mean that it could have had a much larger share for ACO PCPs if they had been more successful.
ACO bonuses may have been lagged out of the analysis. Given that the survey on which the analysis was based was in the field between January 2012 and November 2013, and ACO bonus payments are lagged, it may not have been possible for ACO bonus payments to have played much of a role at the ACO practices at all. Recently, one practice claims to have earned $63K per physician on ACO contract bonuses in the first year (2012). If 30% of this was paid out to the physician as a bonus (generous, given the start-up and ongoing operating costs for an ACO), it would represent a 10% share of typical internist compensation and, if generalized across ACO practices, quite a blip on the author’s regression analysis. However, for 2012 operating year, the bonus was only calculated and issued in 2014, well after the survey window. No wonder ACO payments played no role in incentivizing physicians per the survey.
Written by Tory Wolff