
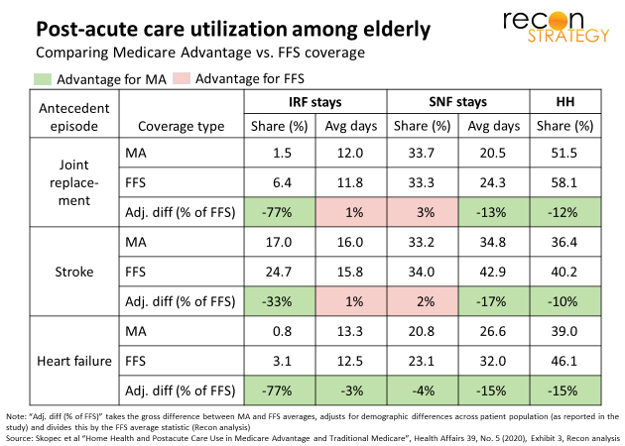
Health Affairs has put out another study – this one by Skopec and team (subscription access) – comparing post-acute care (PAC) among Medicare Advantage (MA) vs. traditional Medicare (FFS). And, once again (see earlier study here – subscription access), we learn that MA beneficiaries use a lot less PAC than FFS with no major differences in outcomes. The pattern varies by type of PAC: far fewer post-acute MA members spend time in an inpatient rehab facility (IRF) but, when they do, they stay just as long as their FFS counterparts; on the other hand, just as many MA members have stays at skilled nursing facilities (SNF) but their stays are much shorter. Notably, the study also found MA members use less home health care vs. FFS which contradicts a hypothesis that MA swaps in home health for facilities-based PAC.
While confirming that greater home health use is not the source of MA advantage, the authors do not surface other explanations. They suggest further research on hidden differences in co-morbidities or unobserved negative clinical outcomes to explain what is going on. The implicit assumption seems to be that FFS is clinically “appropriate” and somehow MA utilization is what needs explaining. And I can understand this view in part: the differences in IRF utilization, in particular, seem peculiarly large without differences in acuity/morbidity playing some role. However, the unadjusted samples seem clinically and demographically well matched. The authors also undertook various statistical manipulations to even out any remaining differences in demographics and hospital/regional variation in care patterns.
Maybe the explanation lies elsewhere. Two possible ideas:
First, managed care may have figured out that PAC does not need to be so intensive or lengthy for many patients. It is well known that PAC is rife unwarranted variation and waste. NaviHealth and Remedy Partners (now merged with Signify) have both built sizeable businesses working the opportunity – NaviHealth largely via MA plans and Remedy largely with providers as part of managing FFS bundles. Their models involve custom PAC plans for each patient and deploying a field force to ensure patients do not get stuck in one setting during their recovery.
Second, managed care may be better at integrating outpatient alternatives in recovery, obviating the need for specialized post-acute support. A closer look at the full picture of care utilization – both outpatient and PAC – across MA and FFS 90 days post discharge will help us understand if managed care is effectively making the swap. Outpatient rehab can deliver great care! The authors note that they could not measure care utilization outside of IRF, SNF and home health so they could not test this hypothesis in this study. That is where I hope the research team will go next rather (than digging deeper into hidden co-morbidities or comparing additional outcome metrics).