
All that effort for only 0.4% savings
Since 2014, HUM has reported on the performance of primary care in value-based arrangements (“VBA”) vs. traditional contracts (“non-VBA”)[1] in Medicare Advantage (MA). One statistic regarding total medical expenditures (TME) is, at first blush, a stunner. The most recent data (2019) shows PMPM TME of VBA members measured only 0.4% less than for non-VBA members. Given HUM’s long-standing strategic commitment to value-based care, commentators are puzzled: is the whole value-based enterprise in vain? does healthcare transformation require quasi-geologic timeframes to deliver meaningful cost impact?
Actually, there is very good news on the VBA impact in the report. The 40-basis point statistic is not an apples-to-apples basis to compare the TMEs of VBA vs. non-VBA. HUM is putting large reductions in reimbursable utilization back into the primary care practices as bonuses. Further, HUM is certainly sharing top-line benefits from Stars performance and risk adjustment documentation with its VBA practices. These bonuses would also be part of TME.
Let’s see if we can use a bit of algebra to tease out what’s going on.
What’s the real difference in reimbursable utilization?
Humana reports VBA practices capturing nearly 2.5x the share of each member’s TME vs. non-VBA practices (~16% vs. 6-7%[2]). Given that PMPM TME for VBA and non-VBA are essentially the same, this data suggests – at a minimum – members are spending a lot more time with primary care than with other forms of care (such as facilities) – something generally applaudable.
HUM also tells us how much VBA practices would be making if their claims were paid under Medicare FFS. Over the last couple years, actual VBA PCP earnings were 1.7-2.5x what they would have earned had their claims been paid under a Medicare FFS arrangement (which is typically the baseline for – or close to – FFS reimbursement in MA). We can use this data as a “deflator” to decompose the primary share of TME into FFS claims “equivalent” reimbursement (normalized to “1”) and VBA bonuses (the “0.7” or “1.5” remaining after subtracting the “1”)
Thus, we learn that 40-60% of what the VBA practices earn was effectively bonus[3], meaning that 5-10% of total TME is a bonus payment to the practices[4]. Removing this bonus would make the TME of VBA 5-10 lower than non-VBA practices on an apples-to-apples basis.
Reconciling the two estimates of TME difference
Only 30% of VBA members are in fully cap deals; the rest are in partial caps and shared savings. Given that, how are VBA practices effectively capturing all the savings? The answer, I think, is in top-line drivers. VBA practices have big roles in closing care gaps and documenting health status, both of which drive plan revenue. HUM suggests VBA practices are delivering on quality: for example, VBA practices had a 0.8-0.9-point lead in HEDIS scores (out of a 5-point scale) in 2016 and 2017, growing to a 1.3-point lead in 2018 (no data for 2019 due to Covid). Risk adjustment is not discussed in the HUM reporting, but it is easy to imagine a strongly performing PCP seeing a 10-15% incremental revenue lift per patient arising from more complete documentation.
Given that, how would the funds flows work out?
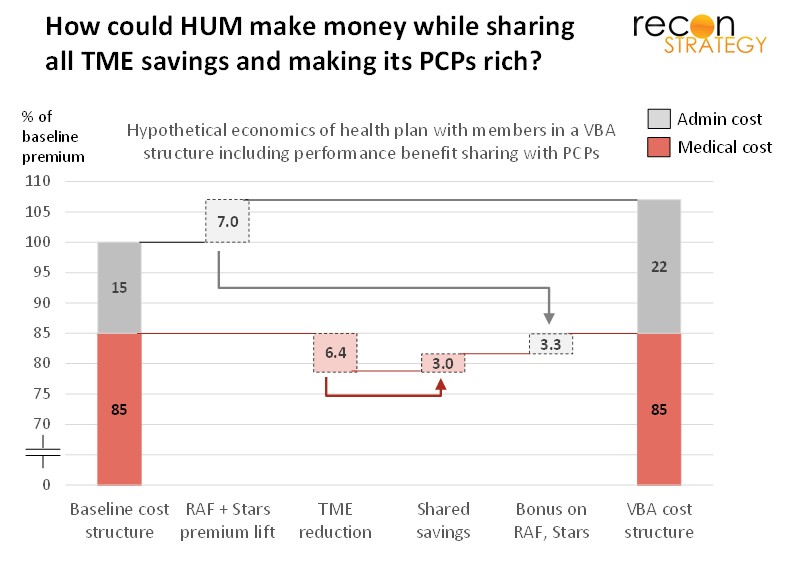
Let’s take 7.5% (midpoint of the 5% and 10%) as the PMPM TME advantage of VBA PCPs vs. non-VBA PCPs. Let’s also rebase this to premiums (rather than TME) assuming an 85% MLR. In that case, 7.5% TME savings would be ~6.4% of premiums. Further, let’s assume fully capitated practices (caring for 30% of VBA members) capture 100% of these savings but the other practices capture in aggregate 25%[5]. That would imply an average 45-50% sharing of cost savings or ~3.0% of each premium dollar. If HUM VBA practices generated the equivalent of a 7.0% topline lift on their members and if HUM shared that gain in the same proportion as savings, the TME advantage would “disappear” – but in fact be alive and well and making both VBA primary care practices and HUM well off[6]. See exhibit:
Big benefits for HUM
Cutting 5-10% out of reimbursable utilization across 2M+ MA lives is a big result (and, of course, not all of this is free margin for primary care physicians[7]). Keep in mind, however, that HUM has had many years to carefully nurture its VBA practices with low membership churn [8].
There are other benefits to a strong VBA program: VBA providers deliver a better patient experience on average, increasing member satisfaction and reducing churn. Further, close alignment between primary care and HUM reduces clinical dissonance and costly appeals, clinical reviews, prior authorizations and so forth. HUM offering an attractive business case for primary care practices also ensures that when practices rationalize their payer contracts, HUM is at the top.
No wonder HUM keeps pushing on VBA.
Implications
- HUM reporting confirms that value-based care transformation – at least as they are running it through their MA book – is delivering reduced reimbursable utilization. In fact, a lot of money can be made in MA by reducing utilization, understanding patients deeply (and documenting what you know) and maximizing quality of care in ways that drive Stars ratings
- The large pool of potential savings gives HUM a lot of resources to solidify ties with top performing primary care practices and provide strong incentives to crowd the members of other MA plans out of patient panels
- MLR floors will ultimately constrain how much HUM can earn on a high performing VBA network. Providers do not, however, face any such constraint. That makes being a top performing primary care practice for HUM an attractive economic proposition, especially if a lot of the non-chargeable services (analytics, tele-engagement, care coordination, etc.) can be consolidated over a larger operating scale. Perhaps this is why HUM is actively investing in primary care assets both via its Partners in Primary Care joint venture and with recently renewed acquisitiveness of its Conviva subsidiary.
[1] VBA care includes any arrangement with shared savings, partial or full capitation components. Non-VBA can be both straight FFS and FFS with pay-for-quality bonuses. About two-thirds of HUM members are being cared for by physicians under VBA arrangements; 30% of these are in capitated arrangements.
[2] HUM also notes that primary care makes up ~4.9% of TME in traditional Medicare FFS (citing Rand).
[3] Bonuses might include performance payments, savings capture, or other higher payments on claims than normally paid by Medicare FFS. Note that the VBA primary care offices are certainly doing more with their patients than what they can submit claims for. Thus, the bonus flows have additional patient touches, incremental utilization and expenses attached to them.
[4] Coincidentally, HUM reporting noted 6% lower inpatient utilization and a 9% lower ED utilization for VBA vs. non-VBA members. Obviously, broader utilization reductions – including outpatient, specialist visits, formulary compliance – would be needed to drive the overall TME reduction. Substitution of specialty and outpatient facilities to the primary care practice likely plays some role here. VBA primary care reimbursable costs repriced at Medicare FFS rates would be the inverse of bonuses (6-9%), about 40-80% more than the typical Medicare FFS primary care share (4.9% of Medicare eligible TME), implying an equally higher amount of reimbursable encounters and services per patient.
[5] HUM reporting notes that 64% of VBA PCPs qualified for savings incentive. Assuming all the capitated PCPs qualified (30%), about half of the remainder (34%/70%) got bonuses. Accordingly, a 25% sharing rate for these practices would imply a roughly 50% sharing rate for practices that earned a bonus.
[6] Note that this is just one scenario. If HUM has lower sharing rates than assumed, then incremental topline lift on VBA practices would need to be higher to achieve the same result. Also, this hypothetical does not factor in MLR floors. Rather than breach these floors, HUM would likely prefer sharing more generously with its providers or invest gains into additional product benefit.
[7] They are certainly doing a lot of non-reimbursable activity to take 6-9% of utilization out of the rest of the system. VBA physicians are likely also trimming panels to spend more time with each VBA patient. But it is hard to imagine all that resulting in a doubling of cost to treat each patient so some of this is real margin for the primary care practices.
[8] HUM has 1.6M MA members with VBA PCPs in 2014 and 2.4M in 2019. Given HUM’s low churn in MA and the pretty high satisfaction VBA PCPs achieve, we can assume the vast majority of those 1.6M are still with HUM in 2019. It is more than likely that least half of the members being treated by VBA practices in 2019 have been with the same PCP for five years, and a much larger share (~80%) for two years.