
Summary
The idea of a single blood-test to detect many cancers is attractive, but is it practical? Can an MCED enhance, or even replace, current screening tests?
This paper delves into these questions by reviewing the effectiveness of current cancer screening methods and identifying areas with the most unmet need. We examine results of Grail’s PATHFINDER2 study on Galleri®, one of the first tools designed to detect many cancers in a single test. However, the test’s adoption will depend on cost-effectiveness, which considers price, cancer detection rate, and associated subsequent diagnostic and clinical care costs.
As Grail and others pursue the pan-cancer approach in ever larger cohorts, we ask ourselves: Should we be screening everyone for every cancer, or is it better to focus on the diseases (or individuals) most likely to succumb to disease?
The state of multi- cancer early detection (MCED) tests today
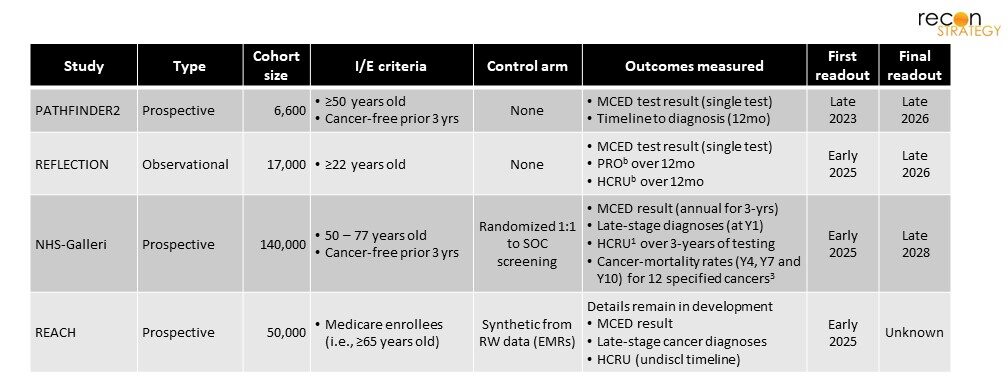
In October of this past year, preliminary results of the first prospective study on a blood test intended for cancer detection were published in the Lancet.1 This is the first, and smallest, in a series of studies sponsored by Grail on the viability and clinical benefit of early-cancer detection by their multi-cancer early detection (MCED) test, Galleri® (Table 1).2 Larger studies aim to determine if use of the test can alter the rate of early-stage disease detection, cancer mortality, morbidity and associated healthcare spending.
More recently, the Molecular and Clinical Genetics Advisory Committee at the FDA held a day-long session to discuss clinical trial designs, importance of tissue-of-origin data, benefits and risks for use in real-world clinical settings.3 As public and private interest in these non-invasive cancer-tests grow, we thought it would be useful to explore both the state of cancer-screening and cancer treatment outcomes today, to understand where a “liquid-biopsy” screening could be a useful addition to preventative care.
Why screen for cancer at all?
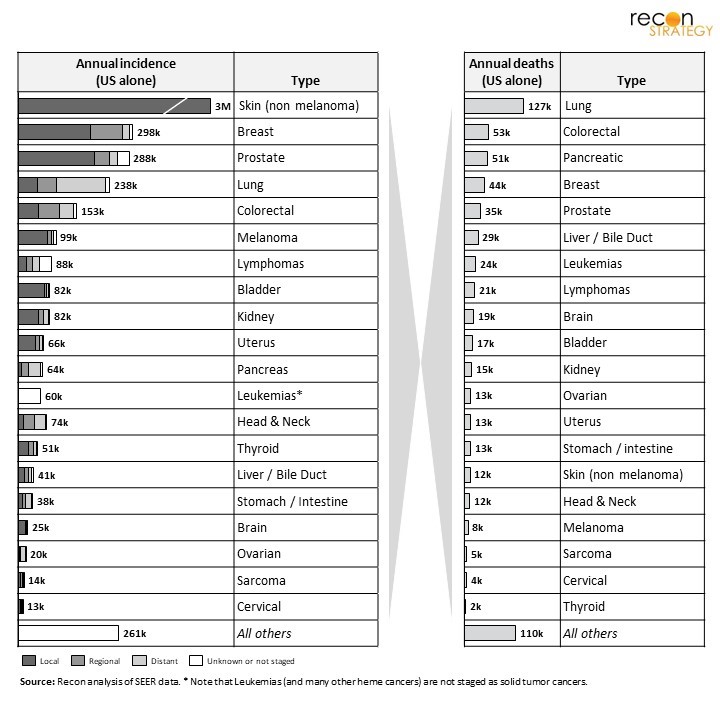
It may seem obvious, but it bears emphasis: the reason we screen for cancers is to reduce cancer mortality and morbidity. That means we don’t just want to find the most common cancers, rather the most common and lethal – which is where the most impact can be had (in terms of lives saved or improved). As can be seen in Figure 1,4 while non-melanoma skin cancer is far-and-away the most common cancer (10x ~higher incidence than the next most common, breast cancer), it is rarely lethal. In fact, if we prioritize by annual deaths, a completely new priority emerges, and the top 3 cancers (lung, colorectal, pancreatic) lead to >37% of all deaths. Of course, lethality is a mix of aggressiveness and stage of disease – and part of the reason lung and pancreatic cancers both float to the top on annual deaths is due to their typically late-stage diagnosis.
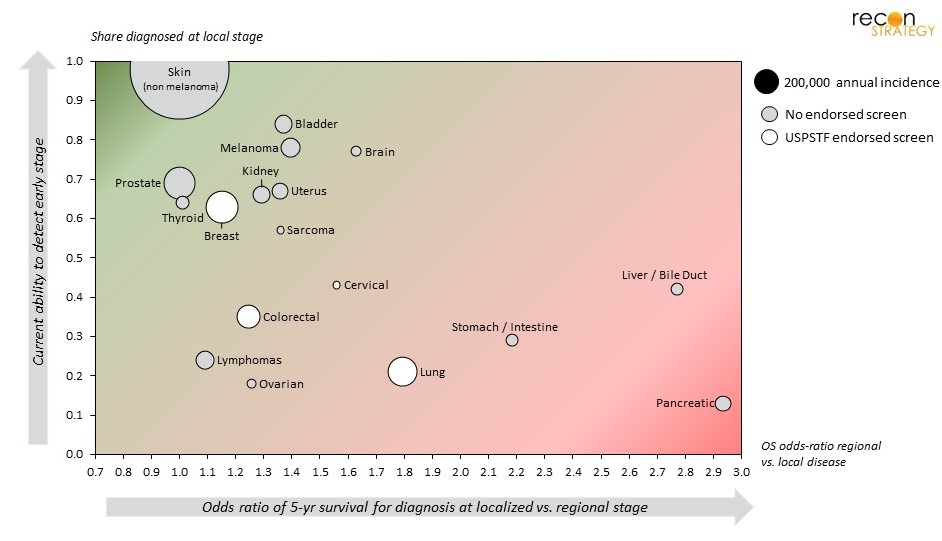
We propose a framework that characterizes not just the number of potential diagnoses, but also the relative unmet need. As shown in Figure 2, comparing lethality of cancer by stage (odds ratio of 5-year survival for local vs. regional diagnoses) against the share of cases diagnosed in early stage, a clear delineation occurs. Diseases in the right half (e.g., pancreatic, liver, stomach, lung) have the worst survival rates, while those on the bottom-half (e.g., colorectal, lung, ovarian) are most often diagnosed in later-stages. The disease most likely to see benefit from increased early-stage detection are those found in the lower-right quadrant (e.g., pancreatic, liver, stomach and lung), with diminishing returns moving toward the top-left quadrant.
A couple of points regarding this framework and the placement of various diseases within it:
- Hematologic malignancies are not staged in the same way as solid tumors. We used regional involvement as a surrogate for lymphomas, but other blood-cancers (including leukemias) cannot be categorized in our approach.
- Impact of existing screening programs on early-stage detection is captured by this framework: y-axis placement (share diagnosed at local stage) reflects both the tests’ innate sensitivity and screening-adherence.
- Carcinoma in situ is a substantial share of “local” breast and bladder cancers (18-25%and 50%, respectively). The value of detection and treatment for these “precancers” is somewhat controversial, particularly in the case of breast (i.e., increased detection and treatment of DCIS in breast has not affected breast cancer survival rates).5
In some cancers, screening programs have already improved diagnosis and outcomes
For cervical, breast, lung and colorectal cancers, the rate of early-stage detection has been improved in recent decades through alternative screening tests, which have been studied extensively.6 As can be seen in Table 2, a range of cancer-screening tests are available. However, not all cancer-screening tests are endorsed by the United States Preventive Services Task Force (USPSTF),7 as not all are believed to offer sufficient clinical benefit. The underlying driver of low clinical value can be due to myriad factors, including:
- Inadequate sensitivity – particularly when an alternative, more sensitive test is available (e.g., chest x-ray vs. LDCT for lung cancer8)
- High false-positive rates where the subsequent diagnostic confirmation is highly invasive and the cancer rare (e.g., CA125 for ovarian, wherein biopsies used for diagnosis can only be obtained surgically9)
- Detecting indolent disease, which leads to treatment of cancers that would otherwise not cause mortality (e.g., prostate,10 thyroid11)
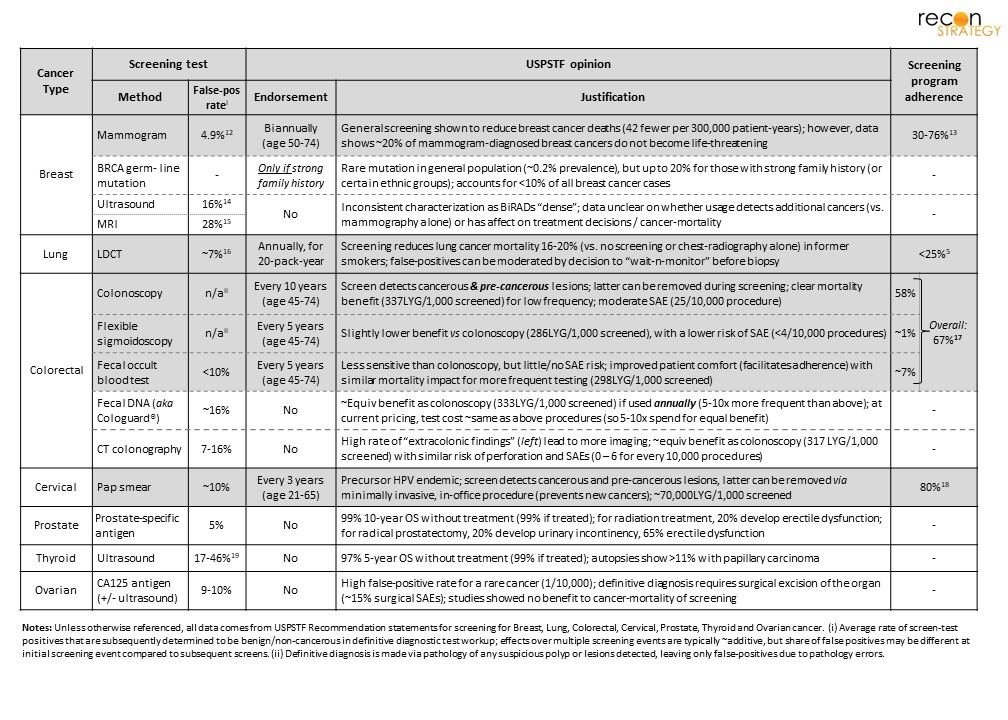
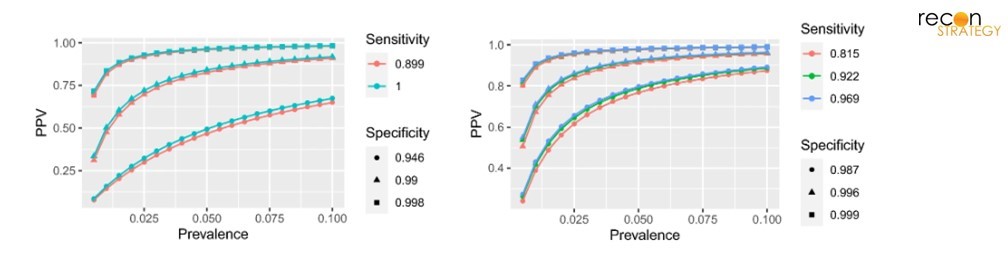
Some of these tests also detect precancerous lesions (e.g., colonoscopy, Pap smear) which can be treated – thereby reducing the incidence for those cancers. However, many also suffer from substantive false-positive rates and adherence is often low. Any test that seeks to replace endorsed programs must improve overall cancer outcomes and spending – and it is important to consider the greater risk of false-positives in low-incidence cancers. As highlighted in Figure 3, (borrowed from Brownstein et al20), the effect means that the cost of follow-up testing will be intensified for the least common cancers. Unless the cost of definitive diagnosis is marginal, this suggests stricter sensitivity/specificity criteria may be appropriate for the rarest diseases (e.g., ovarian, sarcoma).
Grail takes a “blue sky” approach – looking for all cancer-types
Galleri® works by identifying cell-free DNA fragments in blood with unusual methylations, which are indicative of carcinogenicity. Blood-borne DNA fragments can originate from any part of the body, and as a result, this test can detect >50 cancer-types.21 The recent Lancet paper1 study found, over all cancer types, Galleri® had low false-positivity rates (0.9%).22 However, since the level of need varies by cancer (as well as the associated cost and risk of follow-up diagnostic tests), we believe it is crucial to understand performance (both sensitivity and specificity) on a disease-by-disease basis.
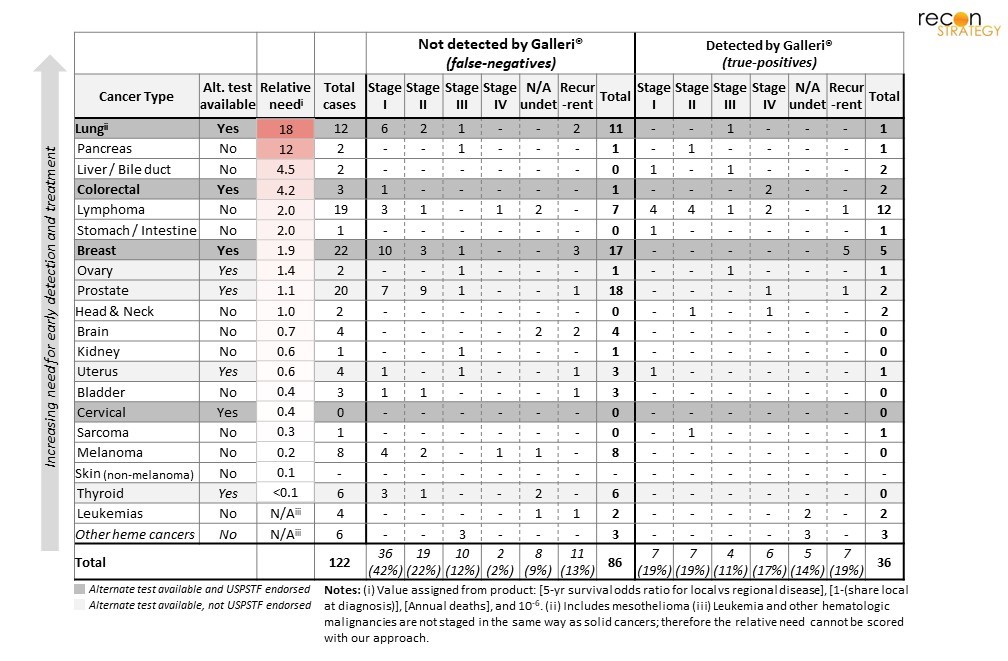
Looking into disease-by-disease results of PATHFINDER2 (Table 3), it quickly becomes clear that much larger cohorts will be needed to observe a substantial number of cancer cases in the general population.23 However, these preliminary results suggest Galleri® is unlikely to replace existing tests – more cancers were seen via standard clinical care and screening (i.e., suggesting a lower sensitivity than existing SOC tools). Even the share of early-stage diagnoses was no better from Galleri® than SOC. Until more definitive data is seen, it seems likely Galleri® will be relegated to being an add-on to existing screening programs and SOC testing. Clearly, the tool can detect diseases which have no effective screening tools today, and even a modest sensitivity here could improve outcomes (e.g., pancreatic, liver and stomach cancer). However, adding this test to clinical practice does have risks: (1) a negative Galleri® test could be used to justify delayed (or non-adherence) screening via more sensitive tests for lung, colorectal or breast cancer, (2) increased general screening will lead to more diagnostic follow-up tests (many of which will turn out to have been false-positives; as discussed above, this will be most common in the rarer cancers).
Will it make sense to add Galleri® (or any MCED) as a screening tool?
Adding a new screening tool comes down to cost effectiveness, which relies heavily on both the test cost and impact on cost/outcomes of subsequent care. This analysis can only be achieved by tracking the total healthcare resource utilization (HCRU), one of the stated goals of both the NHS-Galleri and REACH studies. A recent JAMA24 paper compared the cost effectiveness of colonoscopy vs. a colorectal cancer specific liquid-biopsy (CRC-LB). In brief, this analysis showed CRC-LB in lieu of colonoscopy offered fewer life-year gains (LYG) than colonoscopy alone. While LYG were optimized by CRC-LB used in combination with colonoscopy, the incremental cost effectiveness25 exceeded $350,000 per LYG (at Galleri®’s current commercial price of $949). That is more than 10x the ICER value for colonoscopy alone (<$30,000 per LYG, at an average procedure cost of $1,120);26 the price of CRC-LB must drop to ~$350 to approach equivalent ICER value to colonoscopy.
However, since Galleri®’s intended use is across many cancers, a true cost-analysis must and incorporate the impact across multiple cancers (and surely that is the driver behind the current price-tag). And herein lies the challenge of a broad, pan-cancer approach: many of the rarer cancers occur at such low prevalence that the positive-predictive value of the test is inherently low (i.e., many more false- than true-positives). As a result, many full-diagnostic workups ordered will never yield a cancer to treat, yet still incur substantial HCRU – potentially driving much more added cost than justified by identified cancers and saved lives.
Concluding thoughts
Until the readout from larger studies become available, it is simply too early to comment on whether Galleri® (or other pan-cancer tests) should become a part of routine care. However, it seems surprising that developers have taken the broad, pan-cancer approach, despite vastly different levels of unmet need, different risks of false-positives and inherent predictive value across cancers. Why not first develop a test specific to one of the more lethal asymptomatic diseases (e.g., pancreatic or liver cancer)? Given the rate at which these cancers are found “too late”, and no minimum sensitivity / specificity bar is set by alternate screening methods.
While pan cancer detection may sound revolutionary, and likely appeals more strongly to investors and the general public, getting it implemented is sure to be much harder than tests targeted to a few high-need cancers. When we think of overall impact on outcomes, there is a non-zero risk the pan-cancer approach is net-negative – because despite catching some cancers earlier, it could also worsen outcomes for the most common cancers (e.g., lung breast, colorectal) and adds to total HCRU in follow-up testing for the least-common cancers.
Sarah J. Dolman
Partner
Download a PDF of this article here.
Acknowledgements
The author thanks Abegale McDermott for her assistance in compiling data on alternative cancer screening tests, Marc Herant for valuable debate and discussion of current and future clinical applications, and Jason Brauner for review of this manuscript.
Endnotes
[1] Schrag D, et al. Blood-based tests for multicancer early detection (PATHFINDER): a prospective cohort study. Lancet 2023; 402: 1251–60. doi.org/10.1016/S0140-6736(23)01700-2
[2] (a) Clinicaltrials.gov, NCT05155605; (b) ibid, NCT05205967; HCRU = Health Care Resource Utilization; PROs used assess feasibility and acceptability of Galleri® testing and results, (c) Neal RD, et al. Cell-Free DNA–Based Multi-Cancer Early Detection Test in an Asymptomatic Screening Population (NHS-Galleri): Design of a Pragmatic, Prospective Randomised Controlled Trial. Cancers. 2022; 14(19):4818. doi.org/10.3390/cancers14194818; Cancers evaluated: Lung, Head & Neck, Colorectal, Pancreatic, Myeloma/Plasma-Cell-Neoplasm, Liver/Bile-duct, Stomach, Esophagus, Anus, Lymphoma, Ovary, Bladder. (d) Grail. GRAIL To Initiate REACH Study To Evaluate Clinical Impact Of Galleri® Multi-Cancer Early Detection (MCED) Test Among The Medicare Population. Published November 20, 2023. Accessed December 1, 2023.
[3] (a) Food and Drug Administration, Molecular and Clinical Genetics Panel of the Medical Devices Advisory Committee Meeting Announcement. Published November 29, 2023. Accessed December 1, 2023. (b) Food and Drug Administration, Molecular and Clinical Genetics Panel of the Medical Devices Advisory Committee Meeting 24 Hour Summary Notes. Published December 1, 2023. Accessed December 2, 2023.
[4] National Cancer Institute, SEER Cancer Stat facts. Accessed December 1, 2023. (And links/subpages therein for each cancer type.)
[5] Ward, EM et al. Cancer statistics: Breast cancer in situ. CA: a cancer journal for clinicians 2015, 65(6):481-95. doi:10.3322/caac.21321
[6] For mammography alone, USPSTF recommendations cite dozens of studies that span 10,000s of patients, in both single-arm and SOC-controlled prospective studies, as well as retrospective analysis of real-world outcomes from various healthcare systems.
[7] United States Preventive Services Task Force, Published recommendations. Accessed online December 2, 2023.
[8] Dajac, J et al. To Screen or not to Screen: Low Dose Computed Tomography in Comparison to Chest Radiography or Usual Care in Reducing Morbidity and Mortality from Lung Cancer. Cureus 2016 Apr; 8(4): e589. doi:10.7759/cureus.589
[9] Henderson JT, et al. Screening for Ovarian Cancer: An Updated Evidence Review for the U.S. Preventive Services Task Force. Rockville (MD): Agency for Healthcare Research and Quality (US); February 2018.
[10] Observation-alone has superb outcomes (98% OS after 10-years), yet more than 90% of patients are treated, 15-20% of whom will suffer sexual, urinary, or gastrointestinal side-effects. See: (a) Esserman, LJ et al. Addressing overdiagnosis and overtreatment in cancer: a prescription for change. The Lancet. Oncology 2014, 15(6): e234-42. doi:10.1016/S1470-2045(13)70598-9
[11] Jegerlehner, S et al. Overdiagnosis and overtreatment of thyroid cancer: A population-based temporal trend study. PloS one 2017, 12(6): e0179387. doi:10.1371/journal.pone.0179387
[12] Moss, S., et al. Randomised controlled trial of mammographic screening in women from age 40: results of screening in the first 10 years. Br J Cancer 2005, (92) 949–954. doi.org/10.1038/sj.bjc.6602396
[13] Ferreira, C. S. et al. Breast cancer screening adherence rates and barriers of implementation in ethnic, cultural and religious minorities: A systematic review. Molecular and Clinical Oncology 2021, 15(1): 139. doi:10.3892/mco.2021.2301
[14] Chen, H-L. et al. Comparison of the sensitivity of mammography, ultrasound, magnetic resonance imaging and combinations of these imaging modalities for the detection of small (≤2 cm) breast cancer. Medicine 2021, 100(26): e26531. doi:10.1097/MD.0000000000026531
[15] Myers, KS et al. MRI-guided Breast Biopsy: Outcomes and Impact on Patient Management. Clinical breast cancer 2015, 15(2): 143-52. doi:10.1016/j.clbc.2014.11.003
[16] Silvestri, GA et al. Outcomes From More Than 1 Million People Screened for Lung Cancer With Low-Dose CT Imaging. Chest 2023 164(1): 241-251. doi:10.1016/j.chest.2023.02.003
[17] de Moor, JS et al. Colorectal cancer screening in the United States: Trends from 2008 to 2015 and variation by health insurance coverage. Preventive medicine 2018, 112: 199-206. doi:10.1016/j.ypmed.2018.05.001
[18] National Center for Health Statistics (US). Health, United States, 2015: With Special Feature on Racial and Ethnic Health Disparities. National Center for Health Statistics (US), May Accessed online Dec 2023.
[19] Molnár, K. et al. False-Positive Malignant Diagnosis of Nodule Mimicking Lesions by Computer-Aided Thyroid Nodule Analysis in Clinical Ultrasonography Practice. Diagnostics 2020, 10, 378 doi.org/10.3390/diagnostics10060378
[20] Brownstein, NC, et al. Predictive values, uncertainty, and interpretation of serology tests for the novel coronavirus. Sci Rep 2021, 11, 5491. doi.org/10.1038/s41598-021-84173-1
[21] Grail. What cancers does GalleriⓇ screen for? Accessed online December 2, 2023
[22] The Lancet paper only did not disclose the cancer-site of origin (CSO) for all MCED false-positives, so we cannot comment on implied specificity by disease-type.
[23] This could signal a limitation of GalleriⓇ, or point to a feature of the participant cohort (potentially a more proactive and health care services seeking group than seen on average).
[24] Zainab Aziz, BS et al. Cost-Effectiveness of Blood-Based Biomarkers for Colorectal Cancer Screening—An Ounce of Prevention Is Worth a Pound of Cure. JAMA Netw Open. 2023; 6(11): e2343346. doi:10.1001/jamanetworkopen.2023.43346
[25] Incremental Cost Effectiveness Ratio is defined as [cost(exp-costcontrol]÷[QALYexp-QALYcontrol]
[26] The analysis assumed the sensitivity/specificity reported in preliminary studies (Liu, M C et al. Sensitive and specific multi-cancer detection and localization using methylation signatures in cell-free DNA. Ann Oncol. 2020;31(6):745-759. doi:10.1016/j.annonc.2020.02.011), that used a retrospective cohort heavily enriched in cancer patient samples (>35% of samples from cancer patients).