
In February 2025, the FDA gave IND approval to United Therapeutics for the first xenotransplantation clinical trial, which followed a series of high-profile transplants via the compassionate use pathway from both United and rival eGenesis. Collectively, these milestones have created buzz around the potential for xenotransplantation to address the growing burden of End Stage Kidney Disease (ESKD). However, xenotransplantation is years from approval and widespread use, and the current outlook for a patient looking to receive a human kidney transplant remains sobering. The New York Times recently highlighted stark disparities within the US transplant system, calling for greater transparency and reform in organ allocation and transplant.
In 2022, the US had ~800K patients with ESKD with an annual mortality rate of 14.6%.1 Of these patients, ~550K are on dialysis and ~96K are on the waitlist for a kidney.1,2 Dialysis is a major burden for patients and the US healthcare system with an average annual cost per dialysis patient per year of ~$100K.1 Dialysis severely impacts patients’ quality of life, with in-center hemodialysis patients requiring 4 hours of dialysis 3 times per week.3 The time-consuming nature of treatment in addition to significant financial and symptom burden means that patients on dialysis struggle to maintain jobs and relationships and are often unable to maintain their previous lifestyles.4,5 Transplant significantly diminishes dialysis burden by improving patients’ quality of life and reducing cost associated with dialysis, but with ~96K patients on the waitlist and the number of patients on dialysis continuing to grow, expanding access to transplant is critical to addressing the growing burden and demand. The top-performing countries for transplant in Europe have kidney transplant rates that are comparable to the United States (~55 kidney transplants per million in France compared to ~57 kidney transplants per million in the US); however, given that transplant rates remain low relative to their potential, we believe that there is room for improvement.6 In 2022, a US Senate hearing on the Organ Procurement and Transplantation Network (OPTN) revealed a myriad of problems within the transplant system, including underperformance in capturing potential organ donors, and experts agree that there is room for significant improvement.7 In this piece, we discuss our finding that there may be far more potential organ donors than are currently being pursued by organ procurement organizations (OPOs), and there is room for substantial improvement in overall transplant volume if OPOs pursue more potential donors.
Recent transplant reform
In the US, organ procurement organizations (OPOs) are responsible for identifying potential organ donors, recovering organs from deceased donors for transplant, and coordinating transfer with transplant centers. Recent reform efforts, including Kidney Allocation System Reform, the Increasing Organ Transplant Access Model, and CMS Revisions to Outcome Measure Requirements for OPOs highlight a growing awareness of OPO underperformance and attempt to improve transplant access, and increase transplant volume and quality. The Securing the US Organ Procurement and Transplantation Network (OPTN) Act is more broadly focused on governance of the US transplant system and attempts to end the UNOS monopoly over the OPTN, which is the system that broadly manages organ donation and transplant. The CMS Revisions to Outcome Measure Requirements for OPOs, a 2020 CMS rule change regarding OPO performance evaluation, shows the most potential to directly impact the overall number of donors that are pursued by OPOs.
The 2020 CMS Revisions to the Outcome Measure Requirements for OPOs aims to broaden the donor pool and account for potential donors who were previously unaccounted for by defining donor potential as all inpatient deaths less than 75 years old with a cause of death consistent with organ donation – a far more comprehensive group than the previous definition of eligible deaths, which only includes patients that are legally declared brain dead by state and hospital criteria.8 The new definition of donor potential is used to determine overall donation and transplant rates for individual OPOs, which are then used to rank OPOs and designate them into tiers. The resulting tier system is used to determine recertification on a tier-by-tier basis, as outlined in Figure 1.
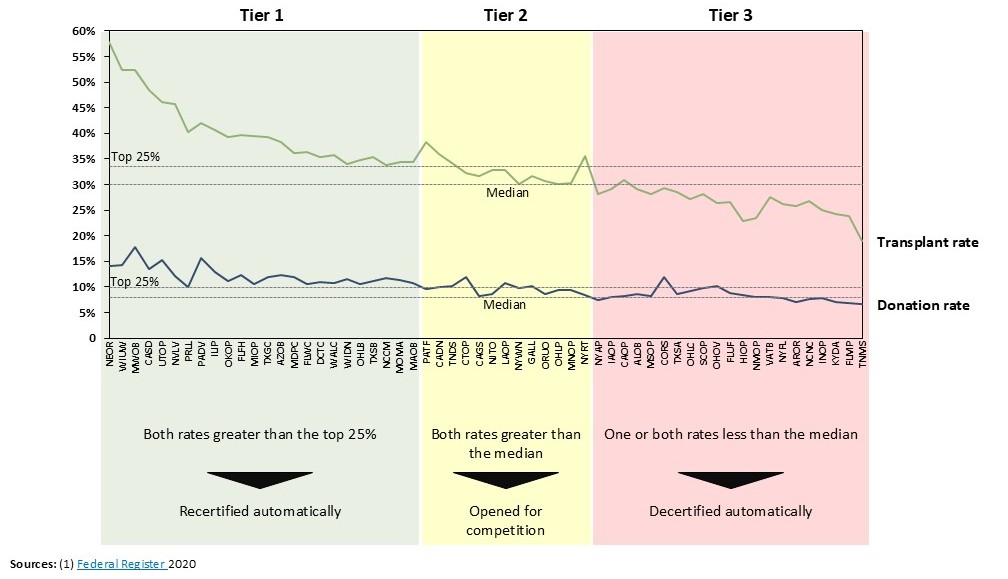
Figure 1. Tier system implemented by CMS to decertify underperforming OPOs.
We note that there is some dissent among transplant experts in the literature around the correct definition of a potential donor. While the CMS definition used in this analysis yields ~100K potential deceased donors in 2022, differing methodologies described by Klassen et al (2016) and Goldberg et al (2017) yield ~50K and ~32K potential donors in 2022, respectively.9,10 Even considering the lower estimates, there were only ~15K deceased donors in 2022, suggesting there is still significant room for improvement regardless of the potential donor definition used.8
Impact of OPO reform on kidney transplants
To understand the potential impact of OPO reform through the newly-implemented tier system, we evaluated how an increase in the number of potential donors pursued by OPOs would change the overall donation rate and number of kidney transplants performed.
The OPO reform introduced by CMS incentivizes OPOs to increase their overall donation and transplant rates to meet the threshold rates of the top 25% performers in order to avoid automatic decertification or competition. Given a 2018 donation rate of ~10.3% across all OPOs and assuming that all tier 2 and tier 3 OPOs reach the threshold donation rate of the top 25% while the tier 1 OPOs continue to improve their donation rates by 25%, we found that the overall average donation rate would increase to ~12.4%. This increase in donation rate would amount to a ~5K increase in total kidney transplants per year by 2030.
Increasing total kidney transplants by ~5K a year is a modest improvement given ~96K waitlisted patients and ~551K patients on dialysis, and a 12.4% donation rate also leaves room for improvement. We found that realistic, incremental improvements on the 12.4% donation rate show potential for more significant impact on waitlisted and dialysis patients. We evaluated the number of transplants at a 15% donation rate, which represents a proportional increase on the CMS reform goal donation rate, mirroring the increase from 10.3% to 12.4%. We also evaluated the number of transplants at a 25% donation rate, which is equivalent to ~50% of the ~50K potential donor estimate noted above, a somewhat conservative estimate of donor potential given CMS’ assumptions. An overall donation rate of 15% would yield an additional ~11K transplants per year, while an overall donation rate of 25% would yield an additional ~35K transplants per year. These estimates for projected increase in overall kidney transplants would be significant, and we found that these changes would have a significant impact on the number of patients on the kidney waitlist.
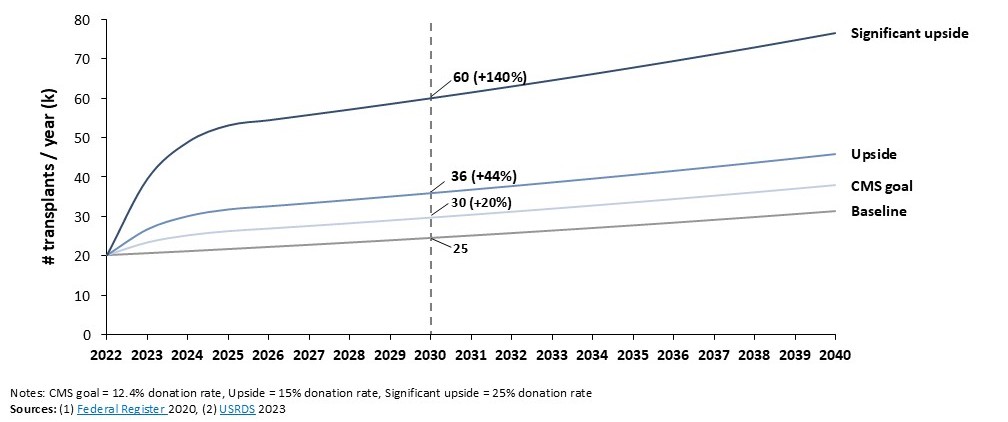
Figure 2. Impact of donation rate on overall number of transplants.
Impact on kidney waitlist and dialysis
In recent years, OPTN data shows the kidney waitlist declining by ~2K patients per year.11 Assuming this is baseline in 2022, by 2030 (or 8 years post-implementation of changes), CMS OPO reform goals show potential to exhaust the waitlist by 2037, whereas at baseline ~60K patients would still remain on the waitlist in 2040. In the upside cases where overall donation rate reaches 15% and 25%, the waitlist would be exhausted by 2031 and 2027, respectively. We note that given a significant increase in the availability of transplants, patients will likely be added to the waitlist at a greater rate than the current rate, so the waitlist will likely take longer to exhaust than modeled in Figure 3.
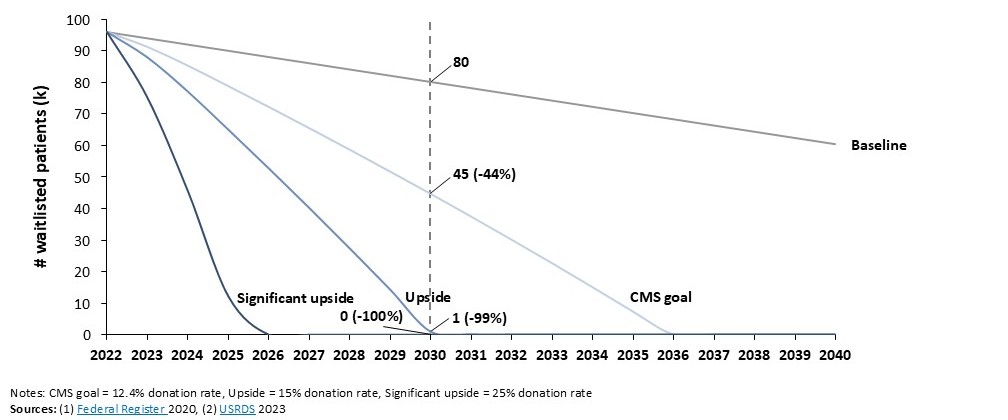
Figure 3. Impact of donation rate on the kidney waitlist.
As the waitlist continues to decline at a faster rate, a new wave of demand for transplants among dialysis patients will likely lead to a significant decline in the number of patients on dialysis. We found that in all cases, an improvement in overall donation rate brings dialysis numbers below the current baseline; however, the number of patients on dialysis falls consistently below current levels only in the significant upside case where the overall donation rate reaches 25%.
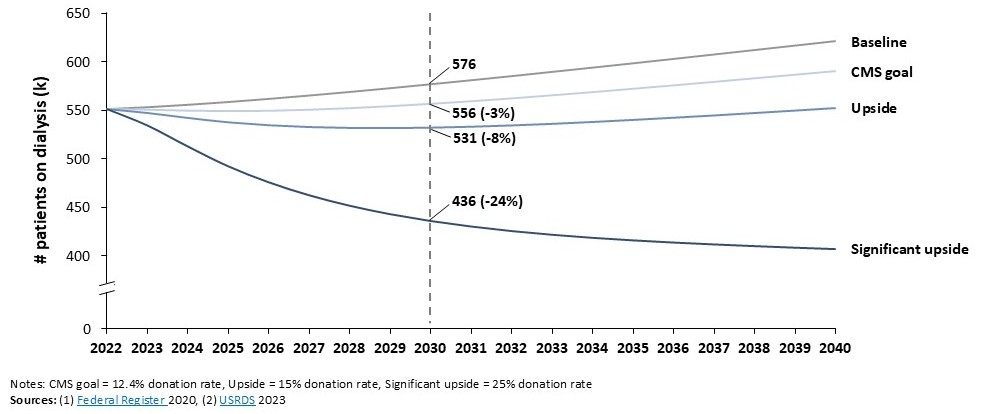
Figure 4. Impact of donation rate on dialysis patients.
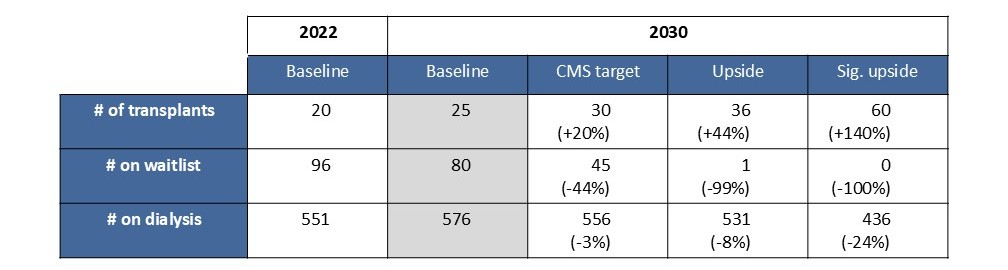
Figure 5. Number (thousands) of kidney transplants, waitlisted patients, and dialysis patients across 4 scenarios.
Future direction
The CMS Revisions to Outcome Measures for OPOs is a step in the right direction to highlight OPO underperformance and incentivize them to capture more donor potential. However, our analysis shows that these new metrics only show incremental improvements in transplant over baseline compared to a significant upside case in which the overall donation rate reaches 25%. In order to make a more immediate and significant impact on dialysis and kidney waitlist, OPOs need to ensure that significantly more potential donors are identified, and all necessary steps are taken to ensure that a potential donor becomes an actual organ donor. Given greater incentives to increase the number of donors pursued and increased accountability and communication among OPO leadership and administration, OPOs may be able to realize much greater donation rates and get patients off of dialysis and off of the kidney waitlist earlier. Further increasing expectations of OPOs by the ESKD community and other stakeholders could accelerate transplantation rates and more rapidly alleviate the growing number of patients on dialysis.
References:
[3] National Kidney Foundation
[4] Al-Mansouri, Asmaa, et al. “Assessment of treatment burden and its impact on quality of life in dialysis-dependent and pre-dialysis chronic kidney disease patients.” Research in Social and Administrative Pharmacy 17.11 (2021): 1937-1944.
[5] Thomas, Sarah T., et al. “Patient and physician perspectives on treatment burden in end-stage kidney disease: a nominal group technique study.” BMJ open 12.12 (2022).
[6] IRODaT February 2021 Report
[7] US OPTN Senate Hearing Memo, 2022
[8] Federal Register: Rule by the Centers for Medicare & Medicaid Services, 2020
[9] Klassen, D. K., et al. “The OPTN deceased donor potential study: implications for policy and practice.” American Journal of Transplantation 16.6 (2016): 1707-1714.
[10] Goldberg, David, et al. “Changing metrics of organ procurement organization performance in order to increase organ donation rates in the United States.” American Journal of Transplantation 17.12 (2017): 3183-3192.