
Earlier this month, researchers released a study of patient-initiated emails to providers with Northern California Kaiser Permanente (KPNC) in 2011/12 in the JAMC . The study focused on patients with one or more chronic condition (CDC data indicates this would be about 50% of an average population) but otherwise sought a mix of conditions, benefit designs and demographics among its participants. Respondents were asked about their use of email in the previous 12 months.
The study found substantial patient initiation of email contacts:
- Of the 71% in the sample with regular access to the internet, 79% said they sent at least 1 secure message to the provider over the past year (56% of the total)
- Among the 56% respondents who emailed providers, 36% (20% of the total) said that emails reduced visits and 42% (24% of the total) said emails reduced calls (or a simple average of 39% substitution rate for visits and calls, implying ~2.6 emails sent for every 1 visit or call avoided).
The cost conscious among us will ask: What do these numbers imply for the overall impact on visits? The number of emails per patient varied (unsurprisingly): Of that 79% with Internet who emailed, 30% emailed 1-2 times; 37% emailed 3-5 times and 33% emailed more than 5 times in the year (17%, 21% and 18% of all chronics respectively). This suggests that the average volume of emails from chronics across an average population was ~1.1 emails PMPY in a year (assuming 17% of chronics sent ~1.5, 21% of chronic sent ~4 and 18% of chronics sent ~6 emails, and assuming that chronics are 50% of the population). Given that 39% of these emails substituted for a visit or call, this volume of emails should in aggregate have substituted for ~0.4 visits/calls PMPY.
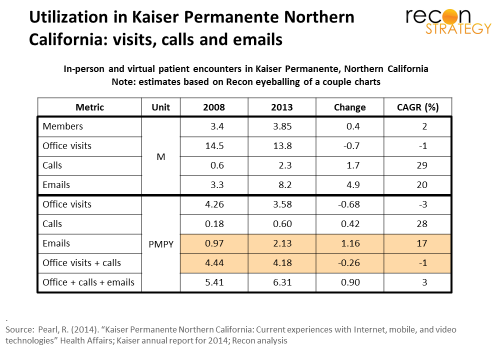
This data can be usefully contrasted with actual utilization data which KPNC separately reported (referred to as HA here). For a summary of results, see exhibit below.
Let’s see if the two sets of data can be reconciled:
- Per the HA data, the overall population at KPNC had 2.1 emails PMPY in 2013, which compares with our estimated 1.1 emails PMPY coming from chronic patients (based on the AJMC data); the difference is presumably made up of emails from patients without chronic conditions. If this analysis is correct, there is no real difference between the email volume generated by healthy vs the sick. This could be a function of demographics (healthier = younger generation = more willing to email) or just that email attracts the contact-needy irrespective of illness status.
- The HA data suggest KPNC has seen a modest reduction in visits PMPY (-3% CAGR) but also large increases in calls and emails PMPY (28% and 17% CAGR respectively). KPNC presumably has strategies (irrespective of email interaction) underway to swap calls for visits. To make this analysis agnostic to those strategies, and, given that the AJMC analysis treats calls and visits similarly, I will aggregate them here. Therefore: excluding emails, total visits and calls declined from 4.44 PMPY in 2008 to 4.18PMPY in 2013 (or about 0.26 PMPY).
- Over that same timeframe, the volume of emails grew by 1.16 PMPY, implying a substitution rate of about 22% (0.26 divided by 1.16). If we assume (per point #1 above) that only 50% of the new email traffic is from chronic members and that, on average, 39% of these resulted in an avoided visit or call, that implies an email-induced reduction in visits/calls by 0.23 PMPY (1.16 x 50% x 39%), very close to the actual reduction of 0.26 visits/calls PMPY. The rest could be explained easily as potential visits of patients devoid of chronic conditions replaced by emails (though, given the similar volume of emails PMPY, implying a far lower substitution rate of about 6% of emails resulting in an avoided visit).
- If this reconciliation is accurate, KPNC providers are responding to 4.5 emails for every call/visit avoided, almost half of them coming from people without chronic conditions but still filling the inboxes (the worried well). Patient initiated emails are not costless to respond to and it is not obvious that responding to 4.5 emails generates lower provider burden than a visit (though operating costs may be lighter for emails).
- Point #3 also assumes all the reduction in visits/calls is a function only of emails. This is unlikely as the period between 2008 and 2013 saw a general tightening of benefit design, increased co-pays and expansion of high deductibles. There are likely a number of drivers for the reduction, not just email substitution, implying that point #4 is overly optimistic and that providers will need to respond to a lot more than 4.5 emails to avoid 1 visit.
Providers are caught a bit between a rock and a hard place. Until an email is defined as a visit with reimbursement and a copay, they must choose whether to offer email as a freebie to reinforce the patient relationship or risk losing the access-sensitive patient to competitors. Local competitive dynamics will likely force each provider’s hand sooner or later. Given that, providers need to be ready to process a large volume of email rapidly (the AJMC data suggest 72% of emails were responded to within 24 hours and another 27% within 1-2 days). If the benefit design is not going to triage the volume (e.g. offering co-pay differentials for patients burdened with a several chronic conditions), the providers must triage at the back-end, perhaps by directing the worried well to physician extenders or RNs and pushing emails from under-managed chronics to the head of the physician’s queue. There’s probably an opportunity to support patient email triage for an entrepreneur.