
(For Louisiana market context, please take a look at previous notes on Ochsner here and here)
Before the holidays, Ochsner signed an LOI to take over the management of ailing University Health located in Shreveport and Monroe and affiliated with LSU Health Sciences Shreveport. The details have yet to be finalized and public disclosure of discussions do not necessarily mean a deal will be made. But Ochsner has been looking at the system for a while and must know its warts and the state appears to have precluded other partnership options. The two other big Louisiana systems – #2 Franciscan Missionaries of Our Lady (FMOL) and #3 Louisiana Children’s Medical Center (LCMC) – claim being denied a chance to make their pitch as alternatives to Ochsner.
Anytime a powerful, fast growing system like Ochsner lands in a new market, it is worth paying attention. When that system – which has been very strategic about rebasing its infrastructure towards outpatient care – is taking on significant inpatient assets, it is worth trying to understand why. Northern Louisiana is far from Ochsner’s New Orleans center of gravity. The Shreveport market is dominated by the competitively aggressive Willis-Knighton system (65% market share measured by admissions) while FMOL leads in Monroe (36% market share). Further, University Health is a legacy safety net system, has been managed since 2013 by an inexperienced operator (Biomedical Research Foundation or BRF), has a toxic relationship with its affiliated medical school and, apparently, deeply troubled finances. Why is Ochsner taking on this headache?
Three reasons:
1. Major opportunity to grow inorganically. The University Health system has about $570M in revenues, 23K discharges and 550 beds (per Medicare cost report data) in markets where Ochsner only has alliances (with Christus in Shreveport with 15% share and IASIS/Glenwood in Monroe with 33% market share). This volume would represent a 20-30% increase over Ochsner’s current system activity. Clinical scale remains a key strategic success factor for nationally ranked systems like Ochsner.
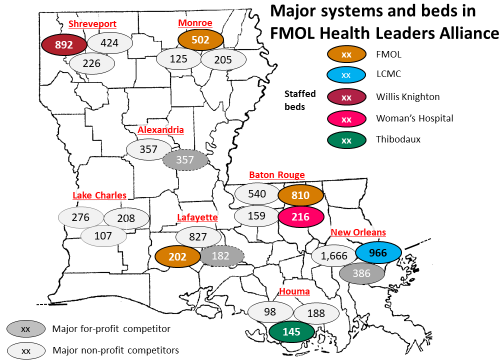
2. Build out of the state network. Ochsner has been building a state-wide clinically integrated network (CIN) since 2014. Shreveport – the #3 city in the state – was a major vulnerability in this network, given the competitive strength of Willis-Knighton relative to the weakness of Ochsner’s local CIN ally Christus. Further, in response to the build out of Ochsner’s CIN, the #2 and #3 systems FMOL and LCMC came together in a competing CIN called the Health Leaders Alliance (HLA). Willis-Knighton was one of the founding members of this network, creating a strong northwestern anchor for the CIN and aligning itself with Ochsner’s major competitors in New Orleans and Baton Route. See exhibit (Note: the bed numbers are adjusted from versions of this map used in previous posts to staffed beds based on data from Medicare data submissions):
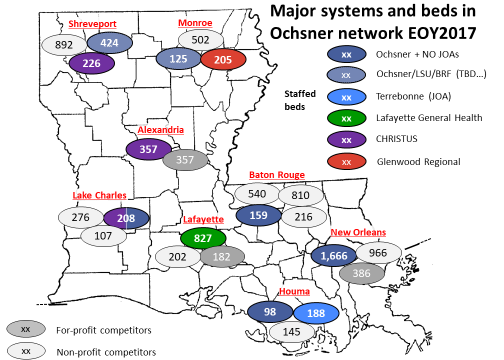
Worse, there were hints that the Shreveport medical school’s frustration with University Health’s current operator was boiling over and it was exploring side collaborations (e.g., opening clinics staffed by LSU Shreveport faculty) with Willis-Knighton. If Ochsner did not seize the opportunity, the University Health system may have fallen into the hands of competitors, be it to Willis Knighton by series of one-off deals or to LCMC or FMOL by a management takeover deal with the state. Instead, if the LOI results in a definitive agreement, the Ochsner Health Network will be in a much better position to compete with HLA in the north. See exhibit (note: the New Orleans Ochsner figures include local systems in neighboring parishes operating under Joint Operating Agreements noted at NO JOAs):
3. Medical school partnership. LSU Health Sciences Shreveport is one of three medical schools in the state. The other two have firm clinical affiliations: Tulane collaborates with HCA in New Orleans (apparently successfully given the joint effort underway to take over the ailing 339-bed East Jefferson hospital); LCMC operates the major teaching hospital affiliated with LSU Health Sciences in New Orleans. If Ochsner wanted a strategic relationship with a medical school to build up its research program, attract more star physicians and sharpen its branding as a leading edge care provider, an affiliation with LSU Shreveport was its local best opportunity .
The move will create significant challenges for Ochsner:
1. Shreveport is remote from New Orleans. University Hospitals in Shreveport is a 4-5 hour drive (250+ miles) from Ochsner’s New Orleans flagship hospital. Currently, the most distant directly run hospital is in Baton Rouge, only 1.5 hours (80 miles) away. I suspect University Health is also remote in terms of operating culture: Ochsner employs all the physicians at its closed-model flagship hospital and about half the physicians staffing the system, has an interesting RVU-based compensation model (per a 2010 report in Health Affairs) and has been investing heavily in its own clinical pathway construction. In contrast, school faculty often struggle with clinical productivity (because of the challenges of juggling the research and teaching missions) and guideline based care (because of natural academic inclination to focus on unusual, interesting cases).
2. Delicate partnership management. With this deal, Ochsner will become a major player in markets where it previously had only allies, creating potential for incentive misalignment. In neither market can Ochsner afford to lose the alliance partner: University Health is too vulnerable to readily stand on its own. Ochsner will need to figure out how to keep incentives aligned. Interestingly (and with fortuitous timing), it has managed to build a model this past summer with Christus in the Lake Charles area: the two combined all their hospital and physician assets into a joint venture. Under the deal, Christus will retain majority ownership and Ochsner will oversee the clinics and affiliated medical groups, as well as invest in access points and sub-specialty care. However, getting partners to agree to such models can be tricky. Baton Rouge General appears to have walked away from a similar deal with Ochsner late last year.
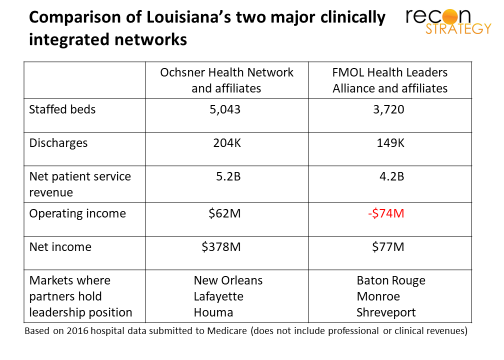
3. Major investments required for the payoff. University Health will need a lot of investments in the physical plant. Faculty have been operating with hiring freezes and other budget restrictions for some time. Further, LSU Shreveport is well behind LSU New Orleans and Tulane in NIH awards and clinical trial activity . To bring the Shreveport medical school up to the nationally ranked standards of Ochsner will take money. But Ochsner’s investment capacity is already stretched with plenty of pre-existing commitments (e.g. to Baton Rouge) and a bond rating below those of FMOL and LCMC (Moody A3 for Ochsner vs. Moody A2 for FMOL and S&P A+ for LCMC).
Despite these challenges, I would bet on Ochsner managing them well. A few items:
- Ochsner has experience working in complex partnerships and scaling its team. It has created and successfully run multiple, flexibly structured joint operating agreements with hospital districts surrounding New Orleans. It has flexed its management team to support new strategies (for example: adding the role of Chief Academic Officer and recruiting Bill McDade from Pritzker in July 2016).
- Ochsner has collected the strongest partners in the state. And competitors are struggling: FMOL economics are weighed down with pension liabilities and the system is in a CEO search. Willis-Knighton is in major management disarray (in October, the system’s medical executive committee asked the system Board of Trustees to replace current CEO Elrod with the then COO; instead, the COO resigned while the CEO promised to launch a search for a near-term successor).
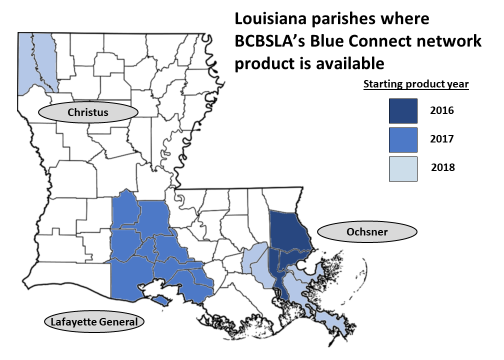
- Ochsner’s CIN is better positioned and appears to be maturing faster than FMOL’s Health Leaders Alliance. Ochsner has had a leadership team for its CIN in place for some time (current CEO David Carmouche has been in the role since early 2016 and COO Sabrina Heltz as COO since July 2016. Both came from BCBSLA) while FMOL is just getting started (Witt/Kiefer appears to have launched the search for HLA’s first senior executive this past November). Further, BCBSLA has been expanding its Blue Connect product around the Ochsner CIN. While the covered lives are likely still relatively small, they have commercial rates and therefore the share gain resulting from this product represent tangible value to OHN partners:
With the takeover of University Health by Ochnser, the Louisiana market structure will be largely fixed. The big switches still to get flipped in Louisiana are Baton Rouge General or BRG (the #2 system in that local market after FMOL and ahead of Ochsner) and HCA in New Orleans (the #3 system behind Ochsner and LCMC in that market – but with the strongest academic positioning with Tulane). I think both systems lack the clinical footprint to thrive in a population-based model. But their strategic paths are unclear: BRG probably can’t align with FMOL without raising antitrust concerns but has already walked away from a deal with Ochsner late in 2016. HCA might face a comparable anti-trust issue aligning with Ochsner in New Orleans but the local alternative LCMC is closely tied with the LSU New Orleans medical school which competes vs. HCA’s Tulane. No good options! When a system like Ochsner is setting the competitive pace in your market, it is wise to move quickly.