
Survivorship care is increasingly pivotal to cancer care delivery and system capacity
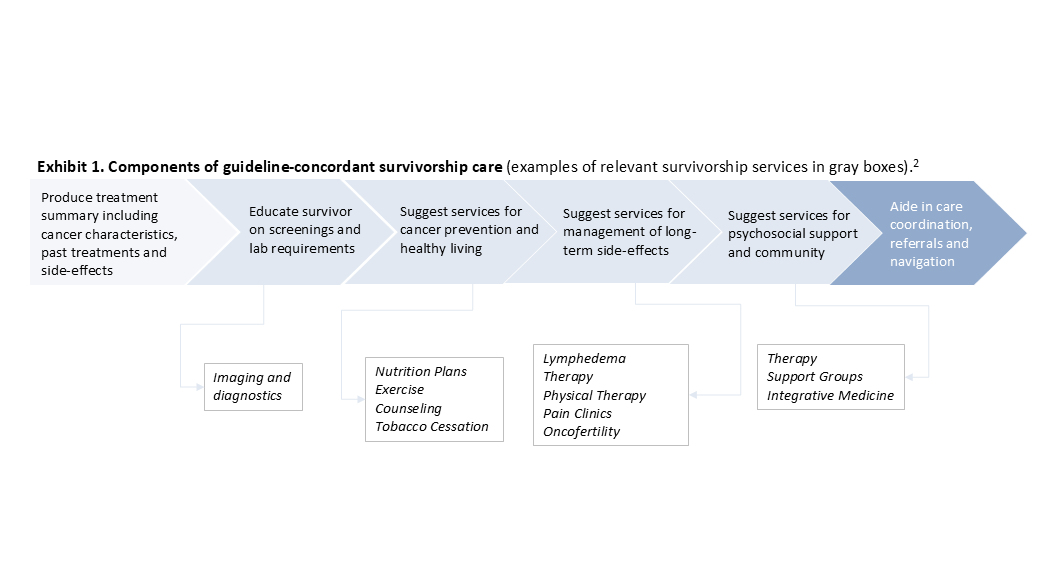
By 2040, 26.1 million Americans will be cancer survivors, representing ~7% of the nation.[1] This is prompting national attention. Oncology guidelines have defined a broad range of supportive services that survivors should receive (See Exhibit 1).[2] In 2020, the Commission on Cancer (CoC) mandated that accredited cancer centers should create dedicated survivorship programs.[3] CMS has also expanded reimbursement of core services such as principal illness navigation (PIN) and care management (PCM).[4]
So far, only 40% of survivors receive a guideline-concordant survivorship care plan (SCP) and only 31% of CoC-accredited centers have implemented dedicated survivorship programs.[5] Closing the survivorship care gap is critical. Questions persist about the optimal approach to survivorship care coordination, timing, workflow, payment, and implementation. This paper explores the emerging approaches being used to structure survivorship and highlights the financial levers that dictate future opportunities in survivorship care.
Cancer centers are moving toward collaborative survivorship models that optimize oncologist capacity.
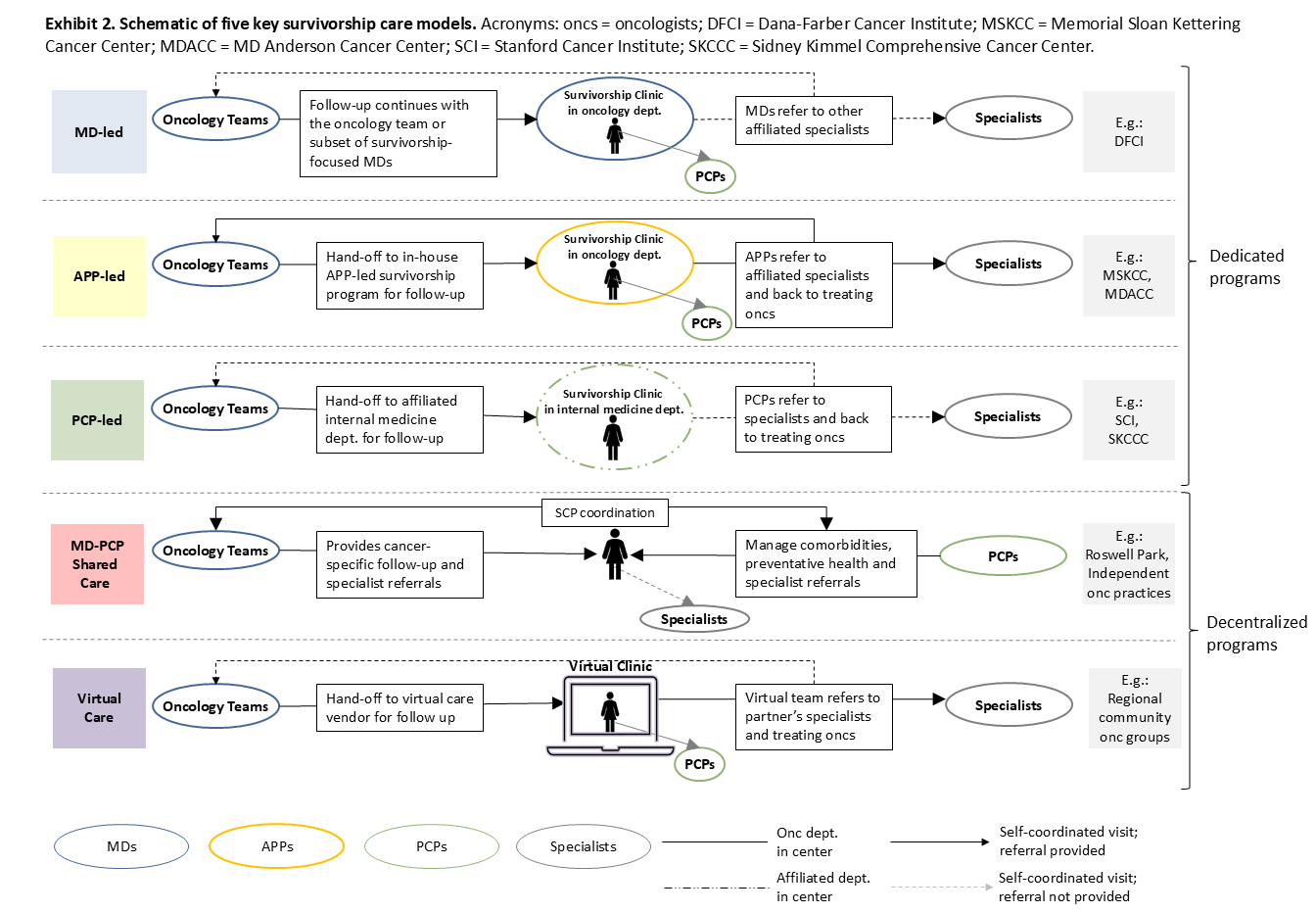
There are five broad models for survivorship care: MD-led, APP-led, PCP-led, MD–PCP shared care, and virtual care (Exhibit 2). The first three function as dedicated programs, where care is delivered either by oncology physicians (MD-led), advanced practice providers (APP-led), or primary care physicians (PCP-led) in an integrated system. The remaining two models, MD–PCP shared care and virtual care, are decentralized. In MD–PCP shared care, follow-up responsibilities are divided between oncology and primary care. Similarly, in virtual care models, portions of follow-up are delegated to external virtual care vendors.
MD-, APP-, and PCP-led dedicated programs are often found in advanced academic centers. When care is managed within oncology settings, APP-led models offer key benefits over MD-led models, such as:
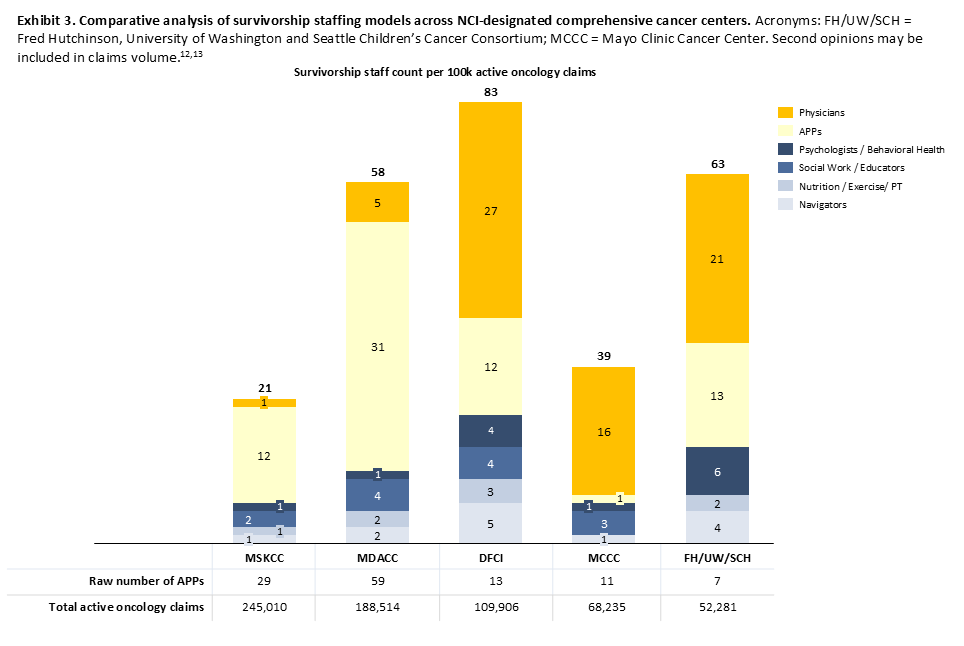
- Increased oncologist capacity to focus on complex or newly diagnosed cases. Our review of staffing at five NCI-designated comprehensive cancer centers (CCCs) supports this idea. CCCs with higher active oncology volume (e.g., MD Anderson, Memorial Sloan Kettering) rely on APP-led models with leaner MD staffing, possibly to expand capacity (Exhibit 3).
- Improved follow-up adherence by keeping survivors connected to familiar members of the care team.
- Maintained financial viability as APP visit reimbursement is generally comparable to physician visits.
PCP-led models, employed by CCCs like Stanford and Johns Hopkins, are driven by a similar rationale to release impending strain on oncology by training internal medicine to conduct stylized survivorship care.[6]
APP- and PCP-led survivorship models offer a promising way to balance oncology capacity. MD Anderson, widely regarded as a lead CCC, has even explored blending the three dedicated models over the last decade through risk-stratified follow-up pathways. Here, survivors are routed to one of either MD-, APP- , or PCP-led care based on the intensity of their clinical needs (see footnotes).[7] While conceptually compelling, evidence on risk-stratified models is nascent.
Experts interviews highlight four key barriers to models led by non-oncologists:
- APPs need the authority to independently order reimbursable tests
- Non-oncology specialists in the system need more survivorship training
- Clear evidence of financial and operational benefits is needed
- Complex patients will need MD-level expertise during follow-up
Outside of integrated CCCs, independent oncology practices often use an MD–PCP shared care approach to balance survivorship care responsibilities. Successful shared care requires strong bidirectional communication between oncology teams and PCPs. Free-standing CCCs, like Roswell Park, use digital tools to generate and share EHR-integrated standardized SCPs that streamline bidirectional communication.[8] They also enroll survivors from the broader community who were treated in other centers via their community networks.
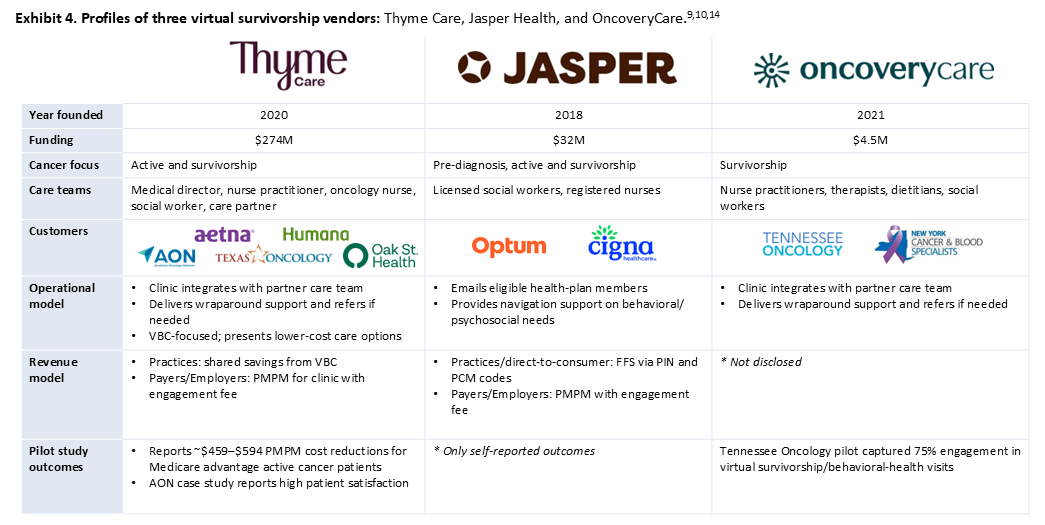
Virtual survivorship models, catalyzed by digital oncology start-ups, are being piloted within regional community oncology groups as another way to manage care demands (See Exhibit 4). [9] Vendors were initially focused on active cancer management for practices and payers, but are now extending into survivorship. Their platforms connect patients to 24/7 virtual care teams with survivorship-trained nurses, social workers, dietitians, and therapists who provide support across four domains:
- Treatment management (symptom management, adherence, care planning)
- Psychosocial health (counseling, support groups)
- Preventive health (exercise and nutrition guidance)
- Care navigation (in-network provider selection and referrals).
Virtual vendors remain early-stage, and greater maturity is needed for broader adoption. Customers and vendor executives highlight four key areas needing development[10]:
- Evidence. Clinicians have concerns that virtual reports over-index on patient-reported outcomes and seek evidence on patient functional gain and cost reduction outcomes from vendor partnerships.
- Integration. Buyers rate vendor EHR interoperability at 6–9/10. While community practices may accept lighter integration, AMCs/CCCs expect deep integration that aligns with center branding and standards.
- Synergistic revenue opportunities. Buyers report limited financial alignment with vendors as they do not share revenue gains from PIN and PCM coding. While larger practices would prefer to outsource this service, it would be a meaningful revenue loss for smaller practices. Former vendor executives also question the financial sustainability of the current volume-based model reliant on PIN and PCM codes.
- Patient engagement. Payer-side buyers note low uptake among eligible members (~20%) and former vendor executives report substantial drop-offs in engagement after the first three months.
As evidenced by the variety of models, survivorship care is non-standardized and highly center-specific. Beyond model choice, approaches also differ in care cadence (episodic vs. longitudinal) and scope (general vs. cancer-specific). Exhibit 5 displays how three key factors – staffing, patient risk, and institutional positioning – drive optimal model choice:

Survivorship care’s sustainability hinges on two economic levers: the external reimbursement landscape and the internal revenue generation opportunities
Historically, survivorship care has been poorly reimbursed with many centers seeking grants or external funding to deliver survivorship services. But there are signals that this is changing. In addition to the 2023 CMS reimbursement change discussed above, evidence-based clinical outcomes of survivorship services will bolster payer interest in reimbursement. For instance, a 2025 NEJM study found that colon cancer survivors who participated in a structured post-chemotherapy exercise program had significantly longer disease-free survival than those who were simply provided educational materials.[11] As survivorship care emerges as a priority, bolstered by clinical evidence, higher reimbursement for survivorship may follow. This would support MD- or APP-led models by increasing the lifetime value of maintaining continuous, in-house follow-up for survivors.
Even under current reimbursement environments, survivorship may still hold internal revenue-generating opportunities for centers via three potential avenues:
- Dedicated survivorship infrastructure expands capacity for higher patient volumes through collaborative care management
- Survivorship services creates downstream revenue by directing survivors to billable supportive services within the center
- Survivorship services creates patient “stickiness” by providing a warm transition to post-treatment care that fosters patient retention and recruitment into the system
Conclusion
Survivorship care is gaining prominence as a clinical and strategic priority. The time is now for cancer centers to decide which model best aligns with their staffing, patient mix and institutional structure. As survivor volumes rise and national standards continue to expand expectations for structured survivorship care, centers that delay survivorship planning risk losing active oncology capacity and falling behind on accreditation and reimbursement shifts. Digital players in survivorship could unlock significant opportunity, provided they bolster their clinical evidence, improve interoperability, and refine partnership and engagement models to better fit clients needs. Early movers will gain a competitive advantage as survivorship becomes an emerging differentiator in oncology care.
References and notes
[1]
- Bluethmann SM, Mariotto AB, Rowland JH. Anticipating the “Silver Tsunami”: Prevalence Trajectories and Comorbidity Burden among Older Cancer Survivors in the United States. Cancer Epidemiol Biomarkers Prev. 2016;25(7):1029-1036. doi:10.1158/1055-9965.EPI-16-0133
- U.S. Census Bureau. Vespa J, Medina L, Armstrong DM. Demographic Turning Points for the United States: Population Projections for 2020 to 2060. Population Estimates and Projections: Current Population Reports. P25-1144. Issued March 2018. Revised February 2020. https://www.census.gov/content/dam/Census/library/publications/2020/demo/p25-1144.pdf
- Tonorezos E, Devasia T, Mariotto AB, et al. Prevalence of cancer survivors in the United States. JNCI: Journal of the National Cancer Institute. 2024;116(11):1784-1790. doi:10.1093/jnci/djae135
[2]
- Rodriguez MA. Care of Cancer Survivors. Presented October 6, 2022. In: OSSN Network NM Inaugural Oncology Conference. American College of Clinical Oncology; 2022. Available at: https://www.accc-cancer.org/docs/ossn-network/nm/meetings/2022-inaugural-oncology-conference-presentations/survivorship_rodriguez-slides.pdf
- McGrath EB. Rural Cancer Survivorship ECHO: The Cancer Continuum. Series July 17-September 25, 2024. Dartmouth-Hitchcock Medical Center; supported by Centers for Disease Control and Prevention. Available at: https://www.dartmouth-hitchcock.org/sites/default/files/2024-10/Rural-Cancer-Survivorship-ECHO.pdf
- Schmidt, R. Survivorship: The Standards of Care. Presented 2022. University of Nebraska Medicine.
[3] Commission on Cancer. Optimal Resources for Cancer Care (2020 Standards). American College of Surgeons. Revised October 2025. https://www.facs.org/quality-programs/cancer-programs/commission-on-cancer/standards-and-resources/2020/access/
[4]
- Centers for Medicare & Medicaid Services. CMS finalizes physician payment rule that advances health equity. Press release. Nov 02 2023. https://www.cms.gov/newsroom/press-releases/cms-finalizes-physician-payment-rule-advances-health-equity
- Nixon Law Group. Additional reimbursement for chronic care management and principal care management finalized in the 2022 MPFS. Nov 5 2021. https://www.nixonlawgroup.com/resources/additional-reimbursement-for-chronic-care-management-and-principal-care-management-finalized-in-the-2022-mpfs
[5]
- National Coalition for Cancer Survivorship. State of Survivorship 2024 Survey. 2024. https://canceradvocacy.org/wp-content/uploads/NCCS-2024-State-of-Survivorship-Detailed-Findings-Final.pdf
- Stal J, Miller KA, Mullett TW, et al. Cancer survivorship care in the United States at facilities accredited by the Commission on Cancer. JAMA Network Open. 2024;7(7):e2418736. doi:10.1001/jamanetworkopen.2024.18736
- Cancer Nation & Edge Research. State of Survivorship 2025 Survey: Detailed Findings. 2025. https://canceradvocacy.org/wp-content/uploads/Cancer-Nation-2025-Survivorship-Survey-Detailed-Findings.pdf
[6]
- Smith SM, Steele N, Kim J, et al. Cancer Survivorship at Stanford Cancer Institute. J Cancer Surviv. 2024;18(1):53-58. doi:10.1007/s11764-023-01523-w
- Choi Y, Radhakrishnan A, Mahabare D, et al. The Johns Hopkins Primary Care for Cancer Survivor Clinic: lessons learned in our first 4 years. J Cancer Surviv. 2020;14(1):19-25. doi:10.1007/s11764-019-00816-3
- Choi Y, Parrillo E, Wenzel J, Grabinski VF, Kabani A, Peairs KS. Optimizing cancer survivorship in primary care: patient experiences from the Johns Hopkins Primary Care for Cancer Survivors clinic. J Cancer Surviv. 2023;17(5):1286-1294.
[7]
- Risk tier criterion: Tier 1 for survivors with very low relapse or late-effect risk after limited, non-intensive treatment; requires prevention and basic surveillance. Tier 2 for survivors with prior multimodal therapy with elevated risk of second malignancies or organ toxicity; requires psychosocial support, internal-medicine specialty care, and selective oncology follow-up. Tier 3 for highest-risk survivors (e.g., high relapse risk, chronic disease, or stem-cell transplant); requires full multidisciplinary, oncology-led follow-up.
- Alfano CM, Suarez-Almazor M, Rodriguez MA, Palos GR, Gilmore KR. Innovating the personalization of stratified survivorship care pathways: using a cancer data ecosystem to improve care access, outcomes, efficiency, and costs. JNCI Monogr. 2021;2021(57):3-9. doi:10.1093/jncimonographs/lgaa011
- Gilmore KR, Rodriguez MA. Identifying optimal program models and clinical tools for follow-up care. JNCI Monogr. 2021;2021(57):18-22. doi:10.1093/jncimonographs/lgab002
- Alfano CM, Mayer DK, Bhatia S, et al. Implementing personalized pathways for cancer follow-up care in the United States: Proceedings from an American Cancer Society-American Society of Clinical Oncology summit. CA Cancer J Clin. 2019;69(3):234-247. doi:10.3322/caac.21558
- Rodriguez MA, Zandstra F. Models of survivorship care. In: Advances in Cancer Survivorship Management. New York, NY: Springer; 2015:7-25. doi:10.1007/978-1-4939-0986-5_2
- Rodriguez MA. Models for multidisciplinary cancer survivorship care. Professional Oncology Education: Survivorship. The University of Texas MD Anderson Cancer Center; 2010. https://streaming.mdanderson.org/transcript/poe-multidisciplinary-cancer-survivorship-care-rodriguez.htm
[8]
- Flores T, Crabtree-Ide CR, Glaser KM, et al. The Cancer Screening and Survivorship Program at Roswell Park Comprehensive Cancer Center. J Cancer Surviv. 2024;18:11-16. doi:10.1007/s11764-023-01521-y
- https://survivorplan.io/
[9]
- Mullangi S, Worland S, Hill B, et al. Association of patient navigation with cancer health spending among Medicare Advantage members: a difference-in-differences analysis. Presented at: 2023 ASCO Quality Care Symposium. Abstract 557. https://20041330.fs1.hubspotusercontent-na1.net/hubfs/20041330/ASCO%20Quality%202023/%5BFinal%5D%20ThymeCare_ASCO23_PosterDigital.pdf?utm_campaign=ASCO%20TCOC%202023&utm_source=ASCO%202023%20Press%20Release
- American Oncology Network. AON and Thyme Care: Enabling Practices with Patient-Centered Support Beyond the Clinic. Case study. 2022. https://www.aoncology.com/wp-content/uploads/2024/02/12466_AON_Thyme-Care_Case-Study_240122_FINAL.pdf
- Graham G, Steele N, Grischkan J, et al. Comprehensive virtual survivorship care: TN Oncology and OncoveryCare Survivorship Program. JCO Oncol Pract. 2025;21(suppl 10):abstr 525. doi:10.1200/OP.2025.21.10_suppl.525. Presented at: 2025 ASCO Quality Care Symposium; Poster Session B; Health Care Access and Disparities Track (Health Promotion Subtrack)
[10] Tegus and expert interviews
[11] Courneya KS, Vardy JL, O’Callaghan CJ, et al. Structured exercise after adjuvant chemotherapy for colon cancer. N Engl J Med. 2025;393(1):13-25. doi:10.1056/NEJMoa2502760.
[12] Definitive Healthcare
[13] LinkedIn
[14] Crunchbase