
This post, by a high school senior who spent the summer with Recon Strategy as a paid intern, explores the literature on doula support for pregnant mothers to complement traditional care to both improve maternal outcomes and reduce costs.
Significant inequalities in US maternal health today
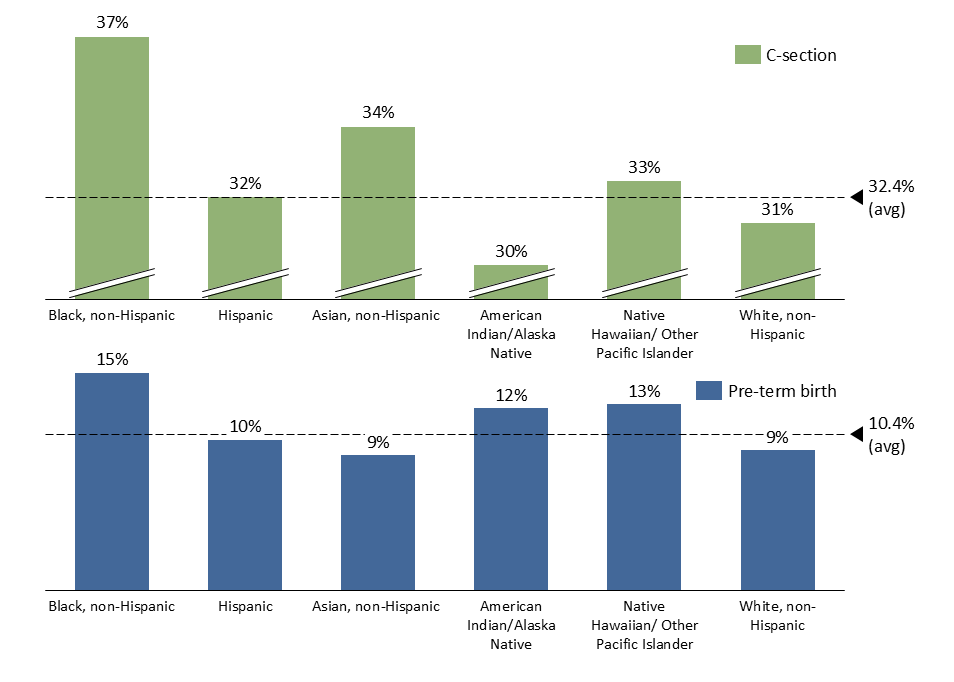
Maternal death rates in the US have more than doubled in the past two decades. Notably, women of color are very overrepresented in this statistic – for instance, black women have higher C-section rates and higher preterm birth rates compared to all other races (Figure 1).
While clinical prenatal care continues to be vital for maternal health, many are starting to think that doula support for pregnant mothers could complement traditional care as a cost-saving intervention that helps improve maternal outcomes.
To explore this opportunity, I reviewed the existing literature on the impact of doulas on maternal care, and trends in coverage within Medicaid plans. I also surveyed 24 doulas to understand their perspectives on doula care.
Doulas: Roles, services, and evidence
According to DONA International, a leading training and certification organization for doulas, a doula is a “trained professional who provides continuous physical, emotional and informational support to their client before, during and shortly after childbirth”. Training, qualifications, and standards are still being developed. Typically, however, doulas provide 2-4 prenatal visits and continuous text support, where education – alongside mental and physical preparation for labor – occurs. Doulas advocate for the mother in the labor room and perform at least one postnatal visit, during which they may refer to other services, such as lactation consultants and mental health specialists.
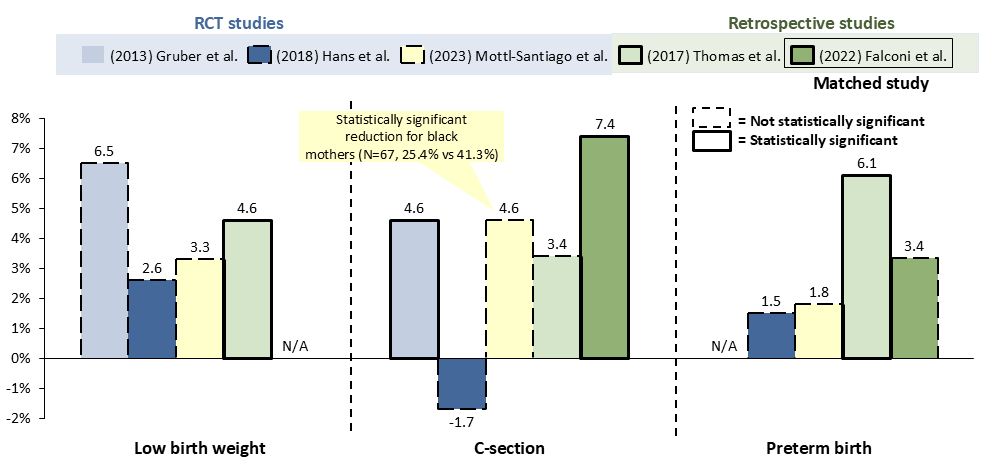
Existing literature suggests that doulas may enable improvements in lowering birth weight, C-section rates, and pre-term birth rates. However, few randomized control trials have been conducted, and retrospective studies often lack well-matched cohorts. While statistical significance was not always achieved, the best quality studies – RCTs or high-quality interventional retrospective studies – generally show that doula care is consistently associated with positive maternal outcomes (Figure 2).
Medicaid programs are initiating doula coverage
In recent years, various state Medicaid programs have become intrigued with the potential value of doulas for populations with lower socioeconomic status. Figure 3 demonstrates state Medicaid programs’ coverage decisions for doulas between 2014 and 2024 (colored green). While some states have not made decisions, they are engaged in active discussions (colored blue). While reimbursement varies from $900-3200, the average in 2024 is around $1200-1600 for a whole birth. Coverage has increased from 2 states with implemented coverage in 2014, to 22 states with implemented coverage and 13 states in active discussions in 2024.
To investigate whether Medicaid’s reimbursement decisions have led to improved doula access, and whether doulas feel they are collaborating successfully with the clinical care team, we surveyed doulas across the US on their perspectives.
Interview findings: doulas and clinical team collaborate well, but ample room to improve
We received survey responses from 24 doulas, with collective experience across 27 states. All surveyed doulas were certified by DONA, and nearly 90% had at least 5 years of experience. On average, they assisted over 50 births each.
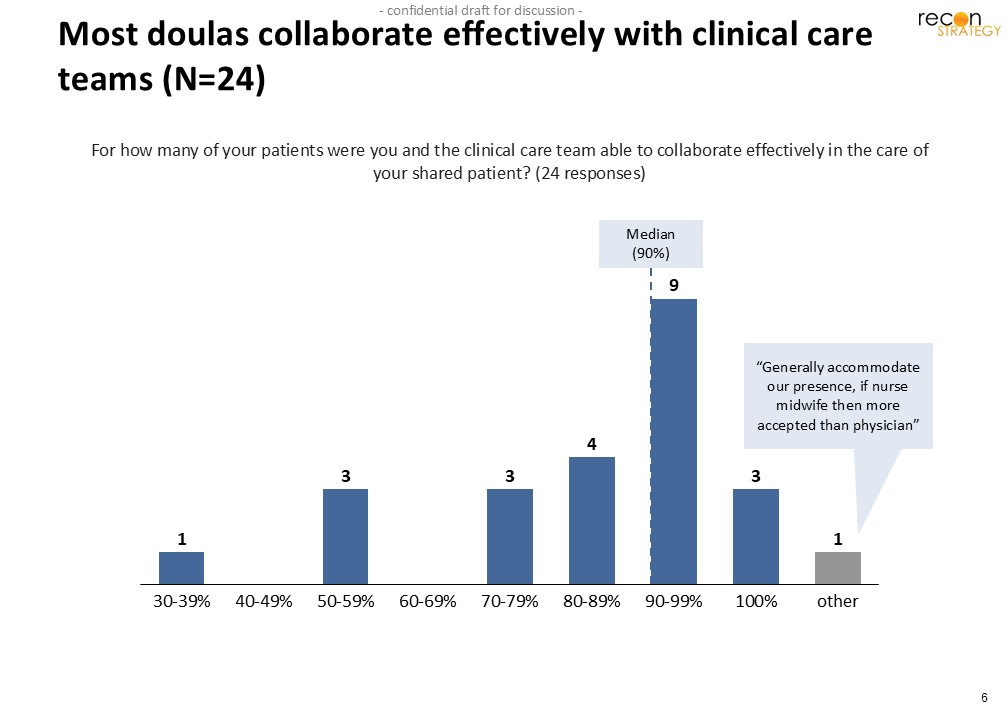
First, we gauged doulas’ experiences collaborating with the clinical care team (Eg: obstetricians, NPs, nurse midwives, anesthesiologists, etc). As seen in Figure 4, the median percentage of patients for which the doula collaborates positively with the care team is 90%. 20/24 doulas report effective collaboration for more than 70% of their patients.
That said, there remains significant room for improvement. Much of the variation may be explained by the operating practices of different systems; one doula described how care differed across two hospitals in the Greater Washington DC area. In her experience, the hospital with a nurse-midwife presence collaborated more effectively with doulas. In contrast, the other hospital’s care teams did not understand the role of a doula, and she felt the care team treated her more as a burden to the care team. Further evidence that systems operating practices can be important can be found in the case of Steward Health. Steward initiated a “Healthy Beginnings” program in 2019, which covers doula care, free childbirth education classes, and other benefits for pregnant Medicaid members. They collaborate and negotiate whole-birth fees with doula organizations. I was told that Steward funded the program in part out of resources supporting its Medicaid Accountable Care Organization operations.
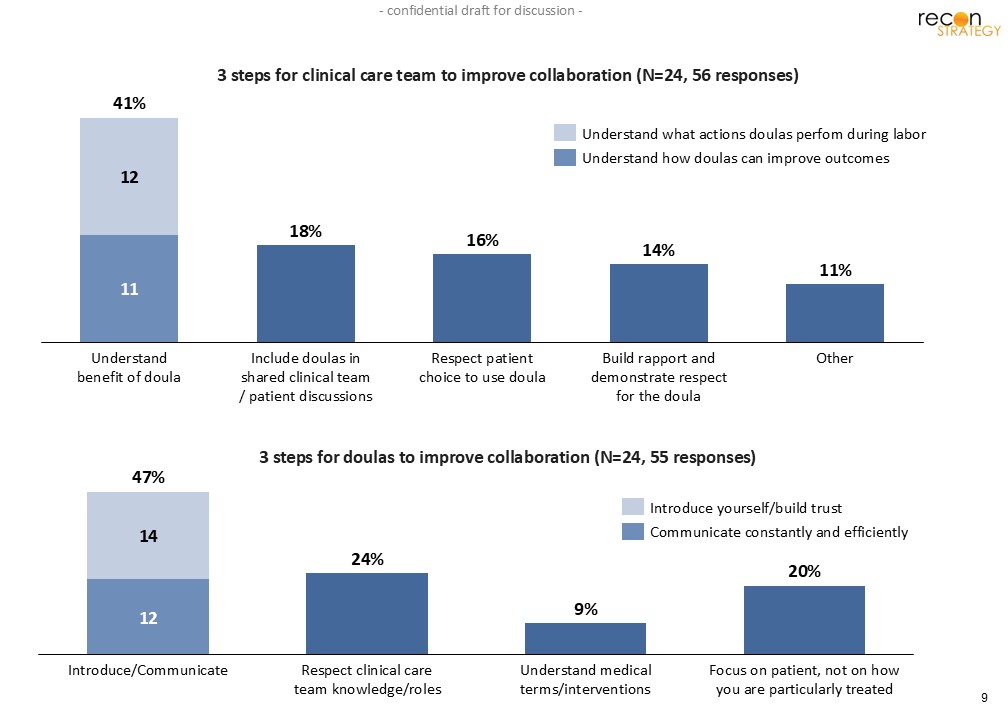
To understand how more effective collaboration can take place, we ask doulas to identify up to 3 steps the clinical care team can undertake. The most mentioned (41%) improvement is understanding the benefit of a doula – both what doulas can do and how they contribute to improved outcomes. After that, doulas recommended that the clinical team include them in shared discussions (18%) and respect patients’ choice to use doulas (16%). Our survey respondents recognized that collaboration is a 2-way street, and also shared ideas on what doulas can take to improve collaboration with the clinical team. The most mentioned steps are introducing themselves and communicating with the clinical team (47%), followed by respecting clinical care team knowledge (24%) and not taking things personally (20%).
In addition to clinical team interactions, we asked doulas about their thoughts on two key questions for optimal care: the role of virtual vs in-person and the best time to initiate the relationship with the expectant mother. These are important questions for health plans to consider when developing reimbursement strategies.
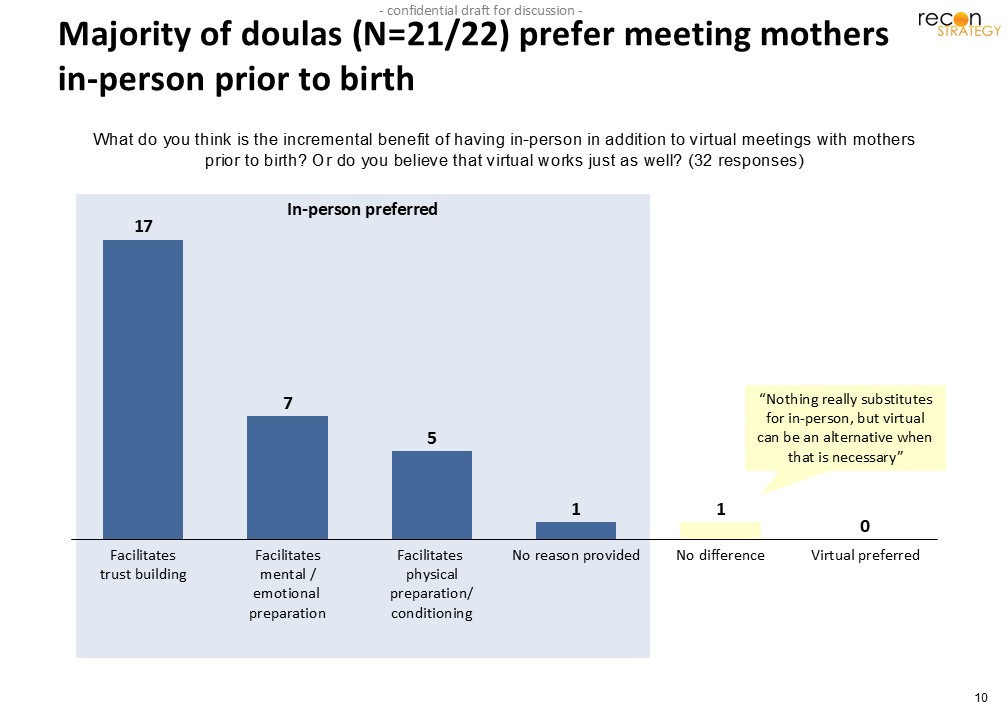
On the first question, the vast majority of surveyed doulas (21/22) preferred in-person interactions, citing the ability to build trust, observe well-being factors (eg: living conditions, availability of healthy food, the smell of smoke) that may impact maternal health, and facilitate physical/emotional well-being by seeing their patients face to face.
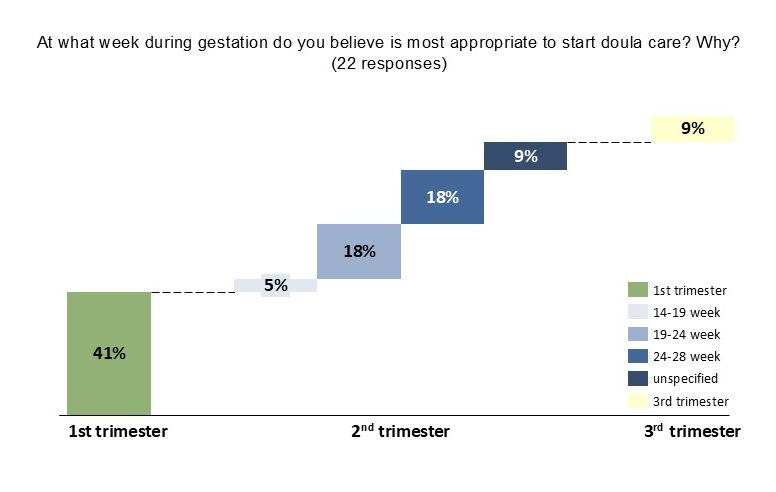
We also learned that most doulas prefer to initiate care during the 2nd trimester, though optimal week-by-week start times vary significantly (Figure 7). However, since outreach is generally driven by the patient, doulas are often not able to initiate care as early as they prefer.
More RCTs, better reimbursement, and better collaboration can help maximize doula value
In conclusion, my analysis suggests that considerable gaps still need to be bridged to maximize the value of doulas. In large part, they stem from limitations in current literature, lack of awareness by clinical care teams on how to effectively collaborate with doulas, and inadequate reimbursement rates provided by state Medicaid programs.
Not enough randomized control trials have been conducted. Many studies fail to offer incentives to retain socioeconomically vulnerable participants. This results in high drop-out rates, which undermine the reliability and statistical significance of data. Future research may benefit from including incentives for remaining in studies such as money, baby toys, and baby clothes – especially for studies targeting vulnerable mothers, who typically benefit most from a doula. Future studies can also benefit from having better-defined recruitment criteria. For instance, many published studies often list “low-income urban mothers”, but do not define what constitutes “urban,” or what income threshold defines a mother as “low-income”.
Another recurring issue is the need for Medicaid plans to match local market conditions when developing reimbursement strategies. Anecdotally, a California doula mentioned that their out-of-pocket clients pay $75/hr for postpartum doula services, but state reimbursement is capped at $3000 for a whole birth. Patients who can pay out-of-pocket end up absorbing the capacity of doulas, leaving few doulas willing to serve disadvantaged populations such as Medicaid recipients in these geographies. While doula reimbursement rates have improved in recent years, further rate increases are necessary to attract doulas to Medicaid clients.
One key limitation of our research was that our survey aimed to explore ways to enhance care collaboration between doulas and clinical teams. However, it would have been more comprehensive if we had also included input from doctors and nurses regarding improving clinical collaboration with doulas.
In conclusion, significant research, improvement in financial incentives, and clinical care team education are imperative to maximize the benefits of doulas.
About the author: Phiona Nabagereka is currently a high school senior attending the Noble and Greenough School. She spent the summer of 2024 with Recon Strategy as a paid intern assigned a project to research doula integration into clinical care teams. Phiona plans to study biology and statistics in college next year, and is considering a career in healthcare.