
Working paper:
Over the coming decades, Alzheimer’s disease threatens to become a huge drag on national well-being. To put things in perspective, by 2040, the US may be allocating more resources to the care of Alzheimer’s patients than care and education of children. Unfortunately, we are not likely to find a therapeutic “silver bullet”; progress will most probably take place in incremental steps as is the case with the latest A-beta directed therapies. Because of the potential modest benefit of new individual therapies, one could reasonably argue to place stringent limits on the utilization and economic pay-off of such outcomes from R&D efforts. We suggest that would be a detrimental for two main reasons. First, that meaningful change in the course of Alzheimer’s will likely require stacking multiple therapies, and the time to build that stack is now. Second, given the risk of failure and the amount of time and investment required, the reward incentives for even a modest positive outcome of an R&D program in Alzheimer’s need to be substantial; otherwise, investment in biopharma pursuing Alzheimer’s will flag. Finally, we show using the example of advanced prostate cancer how over the past two decades, a series of therapies each showing modest improvements over the prior standard of care have led to meaningful overall progress with good value for money in the long run despite high costs in the short run.
Beyond a heavy burden on individuals, Alzheimer’s disease represents a substantial threat to US social well-being overall
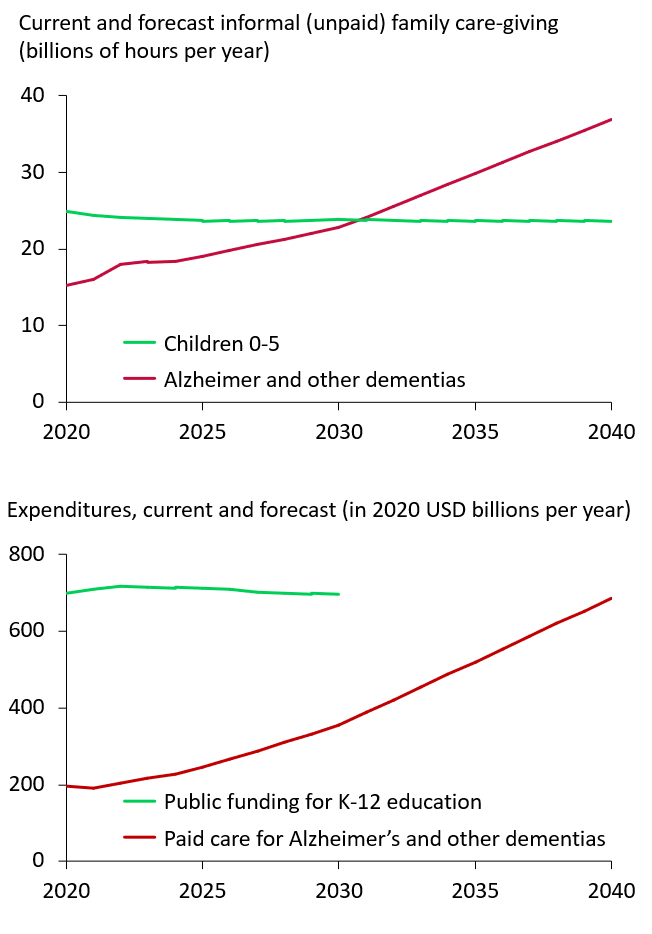
Alzheimer’s disease (AD) is poised to become a massive societal burden. The greatest risk factor for developing AD is age, and the youngest of the baby boomer generation will have reached 65 years old by 2030. In 2023, an estimated 6.9 million adults over 65 had AD in the US; this number is projected to grow to 11.16 million in 2040 (Alzheimer’s Association Facts and Figures, 2024, Rajan et al, 2021)[1][2]. Today, much of the caretaking burden of dementia (of which AD is responsible for 60-80% of cases) is borne by informal caretakers (Sosa-Ortiz et al, 2012)[3]. The mean survival time for patients with AD is 5-8 years post diagnosis (Liang et al, 2021)[4]; this also doesn’t account for the years of mild cognitive impairment (MCI) that predate formal AD. As the demographic shift occurs, AD caretaking will present a tremendous strain on working-age adults. In coming years, the informal caretaking role of adults will shift from the young to the elderly. Combining data from the US Bureau of Labor Statistics[5] in conjunction with population[6] and family living arrangement[7][8] estimates from the US Census Bureau, hours of informal caretaking for AD and other dementia patients will overtake the hours families spend caring for their children 0-5 years in about a decade (Exhibit 1).
The cost of formal care for AD will also pose an economic burden. Projected spending on formal care for AD and other dementias was $196 billion in 2020 and will rise to $1.4 trillion in 2060 (Nandi et al, 2024)[9]. This will soon catch up to the entirety of public-school expenditures for K-12 students in the US (National Center for Education Statistics 2022-2030 projections)[10] (Exhibit 1). Generally, future healthcare expenditures will include age-related spending as part of a national pattern of resource use.
Without progress in therapeutic interventions to lessen the demands of AD, the burden on US society risks becoming dramatic, to the point that it will color all aspects of everyday life.
Progress against Alzheimer’s is likely to continue to be slow, incremental and with many failures
It is remarkable that although the characterization of Alzheimer’s disease by Alois Alzheimer and his peers of the early 1900s already identified the two key elements of the pathophysiology (plaques and tangles) that continue to be the main focus today, an intervening century of research has not led to an elucidation of the root processes of Alzheimer’s disease.[11] This incomplete understanding of the mechanism(s?) of disease together with the lack of good animal models has profoundly impeded progress in the search for therapeutics.
To put things into perspective, in the modern era, more than 200 drugs have been put in human trials for Alzheimer’s disease and failed to show therapeutic benefit. Compare that with the less than 10 that have obtained approval for Alzheimer’s in the same period, of which only three are thought to potentially act by modifying the underlying disease course rather than improving symptoms. Looking ahead, the path does not look less arduous because basic research has not been able to yield breakthroughs in our understanding of disease biology. If anything, the process is working backward – it is thanks to trying every permutation of A-beta directed therapies in the clinic that we now believe that oligomers are the most neurotoxic species playing a role in neurodegeneration.
Unfortunately, this makes it unlikely that a silver bullet therapeutic will emerge against Alzheimer’s. The more likely outcome is similar to many other conditions where a stacking of interventions gradually moves the needle over a long period of incremental progress. Drugs like Leqembi and Kisunla which act on the pathophysiology of early Alzheimer’s disease with modest impact on its clinical manifestations are likely the first steps in the long series that will be needed to address this disease. Despite the modest clinical impact, the total cost of Leqembi (which currently is prescribed for an indefinite duration), including scans, procedure cost, etc. is estimated to be 109k (Institute for Clinical and Economic Review, 2023[12]). Kisunla, which can be stopped if certain thresholds for decreased amyloid beta in the brain are met, could potentially cost somewhat less on a per patient basis.
Progress step by step: the example of metastatic prostate cancer
Advanced prostate cancer that has escaped control with traditional hormonal therapy typically leads to death within 1-2 years. Over the last two decades a series of novel agents have been developed and tested in the clinic and have been found to extend survival (Exhibit 2)
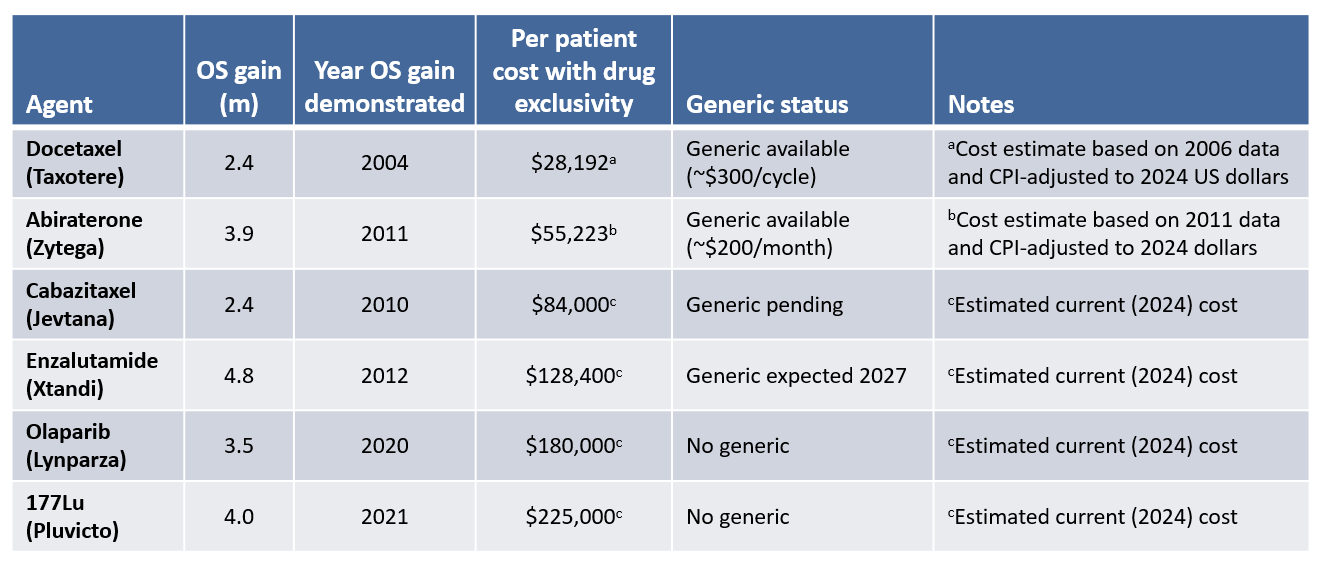
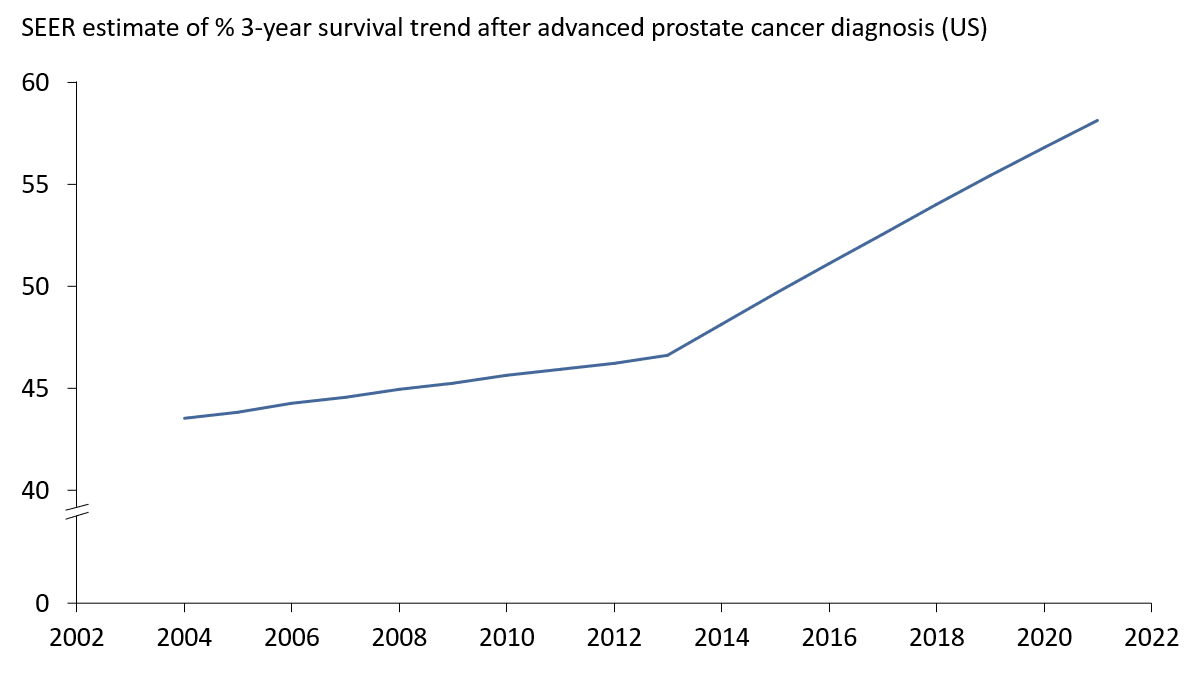
Unfortunately, each agent only leads to a modest gain in life expectancy of a few months at most (though to be fair, they also improve other aspects of the disease such as pain). This reflects how, despite best efforts to devise new therapies, advanced prostate cancer is a very challenging disease to address. However, over decades, these incremental benefits add up to meaningful progress in the survival rate as seen in the overall US survival data (Exhibit 3).
While under exclusivity, these agents are or have been expensive, and it is possible for a reasonable person to argue that the cost is beyond the value delivered to the patients. Two counter-arguments make the reverse case.
First, the exclusivity period is finite, and once a generic enters the market, then the value delivered is truly outstanding, and indefinitely so. In the case of docetaxel and abiraterone, the cost now is likely less than $1,000 per month of life gained.
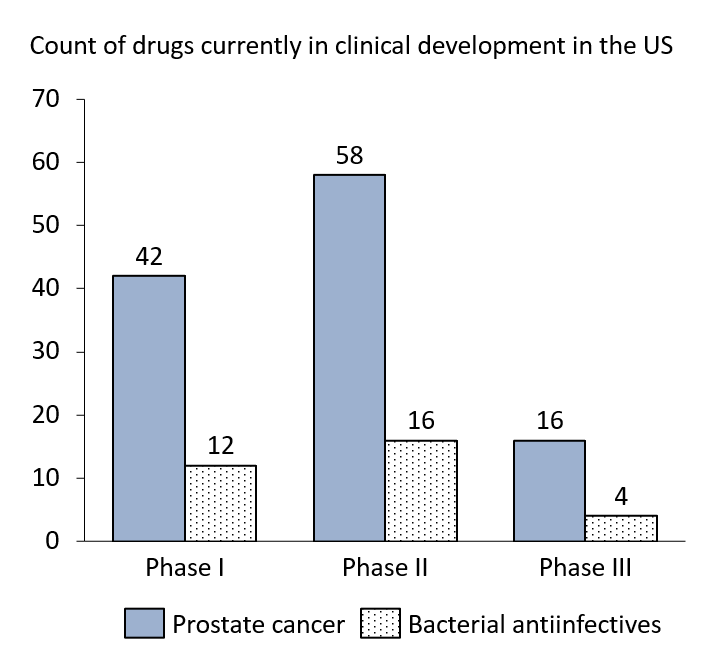
Second, these high prices are the reason there are more than 100 drugs in clinical development for prostate cancer in the US; most of these drugs will fail and never be approved for prostate cancer. But investors in biopharma companies have made the decision that the shot is worth the risk, because the economic reward for success, even modest, has been historically substantial. But should that reward shrink markedly, investors will take their money elsewhere, and it is easy to see a world where the number of drugs in the prostate cancer pipeline diminishes dramatically.
A simple comparison tells the story, consider bacterial anti-infectives; despite major concerns about “superbugs”, R&D activity remains low because the use of any truly novel agent will be limited to those cases that really need it due to the fear of emergence of resistance, or, in other words, a very small market with limited economic rewards (Exhibit 4).[13]
Discussion: policy trade-offs and progress in Alzheimer’s disease
A recurrent tension in public policy is the question of whether to allocate resources for well-being today, or for investments that will improve well-being tomorrow. Some elements of this trade-off are personal and societal value judgments, but others are more quantifiable (how much investment for how much improvement, and how soon, and for what broader social impact).
How are those trade-offs made on progress in finding new drugs to treat disease? We live in a world where 99% of new drugs are discovered and developed by for-profit entities with investors who have many other options on where to allocate their money. One could envision different models, e.g. such as state-managed endeavors, but there is no serious proposal to change our pharmaceutical R&D model on the table today. As a result, a key driver of therapeutic innovation is that of economic incentives: the prospect of rich rewards for a drug that works attracts more R&D investment, the reverse decreases it.
Those incentives happen to be for a large part in the hands of government: at the regulatory level (e.g. FDA), the legislative level (e.g. intellectual property regimes, agency mandates), and at the budgetary level (e.g. drug reimbursement in public programs). Therefore, in essence, government makes the trade-offs: e.g. less reimbursement for new drugs means more money to do other things, but less incentive for drug R&D, and the reverse is true.
In the case of prostate cancer, maintaining high incentives for further R&D via generous economic terms for new drugs has improved the lives of many patients and their immediate families but the broader social impact is limited. A change in incentives (e.g. through the IRA drug legislation or the like) may inflect the rate of progress in prostate cancer, but even if it does, it is a trade-off on which one can reasonably have a range of opinions: less expensive drugs today for less progress for tomorrow vs. more expensive drugs today for more progress tomorrow.
However, the case of Alzheimer’s is different. With a tidal wave of burden that is approaching the US, the need for Alzheimer’s therapies takes a national dimension with large scale societal stakes. Our argument here is that if there is one therapeutic area where the trade-off of incentives for progress for tomorrow vs. savings for today should prioritize progress, it is Alzheimer’s. In that respect the experience with Leqembi and Kisunla will be very important. Here are two drugs with modest but well validated clinical benefit – a result which any company with current R&D in Alzheimer’s would be ecstatic to achieve. If these drugs fail economically because of policy choices (low reimbursement of the drugs or related care processes, e.g. imaging), then the message to Alzheimer R&D will be: only therapies that have a major impact on the disease will be rewarded. The impact on R&D incentives would be significant: instead of a probability of success for a program of a few %, investors would be looking at a probability of success in the sub-1% level (based on historic patterns), and most would simply invest elsewhere.
Given the history of the field, progress against Alzheimer’s is likely to take place in steps that are small, and that each take major risk and effort. But if incentives are not there for the R&D enterprise, the potential is there that these steps won’t be taken, or not taken soon enough to mitigate the burdens we will face as a society in the next decades.
References:
[1] 2024 Alzheimer’s disease facts and figures. Alzheimer’s Dement., 2024; 20: 3708-3821. https://doi.org/10.1002/alz.13809
[2] Rajan KB, Weuve J, Barnes LL, et al. Population estimate of people with clinical Alzheimer’s disease and mild cognitive impairment in the United States (2020–2060). Alzheimer’s Dement. 2021; 17: 1966–1975.
[3] Sosa-Ortiz, A. L., Acosta-Castillo, I., & Prince, M. J. (2012). Epidemiology of Dementias and Alzheimer’s Disease. Archives of Medical Research, 43(8), 600–608. https://doi.org/10.1016/j.arcmed.2012.11.003
[4] Liang, C.-S., et al. (2021). Mortality rates in Alzheimer’s disease and non-Alzheimer’s dementias: a systematic review and meta-analysis. The Lancet Healthy Longevity, 2(8), e479–e488. https://doi.org/10.1016/S2666-7568(21)00140-9
[5] Average hours per day parents spent caring for and helping household children as their main activity. (n.d.). Bureau of Labor Statistics. Retrieved from https://www.bls.gov/charts/american-time-use/activity-by-parent.htm
[6] U.S. Census Bureau (2023). National Population Projections Tables: Main Series. Retrieved from https://www.census.gov/data/tables/2023/demo/popproj/2023-summary-tables.html
[7] U.S. Census Bureau. (2021). GRANDCHILDREN UNDER 18 YEARS LIVING WITH A GRANDPARENT HOUSEHOLDER BY AGE OF GRANDCHILD. American Community Survey, ACS 1-Year Estimates Detailed Tables, Table B10001. Retrieved September 20, 2024, from https://data.census.gov/table/ACSDT1Y2021.B10001?q=ACSDT1Y2018.B10001&g=010XX00US
[8] 2023 Current Population Survey Annual Social and Economic Supplement, America’s Families and Living Arrangements Package, Table A3, https://www.census.gov/data/tables/2023/demo/families/cps-2023.html
[9] Nandi, A., Counts, N., Bröker, J., Malik, S., Chen, S., Han, R., Klusty, J., Seligman, B., Tortorice, D., Vigo, D., & Bloom, D. E. (2024). Cost of care for Alzheimer’s disease and related dementias in the United States: 2016 to 2060. Npj Aging, 10(1), 13. https://doi.org/10.1038/s41514-024-00136-6
[10] U.S. Department of Education, National Center for Education Statistics, Common Core of Data (CCD), “National Public Education Financial Survey,” 1989-90 through 2018-19; National Elementary and Secondary Enrollment Projection Model, through 2030; and Public Elementary and Secondary Education Current Expenditure Projection Model, through 2030-31
[11] Korczyn, Amos D., and Lea T. Grinberg. “Is Alzheimer disease a disease?” Nature Reviews Neurology 20.4 (2024): 245-251.
[12] Lin GA, Whittington MD, Wright A, Agboola F, Herron-Smith S, Pearson SD, Rind DM. Beta-Amyloid Antibodies for Early Alzheimer’s Disease: Effectiveness and Value; Evidence Report. Institute for Clinical and Economic Review, April 17, 2023. https://icer.org/assessment/alzheimers-disease-2022/#timeline
[13] Plackett, Benjamin. “Why big pharma has abandoned antibiotics.” Nature 586.7830 (2020): S50-S50.