
For years, digital biomarkers have seemed like a promising way to transform drug clinical trials, yet their adoption journey has been uneven. We’ve watched as the excitement for Proteus’s ingestible sensors dissolved when the company filed for bankruptcy. We’ve seen major investments to build large and sophisticated digital health teams by biopharma companies (e.g., Biogen) lose steam. Yet, as we enter 2025, there seems to be a renewed sense of optimism among digital health innovators and trial sponsors accompanied by positive indicators from regulators. This is why AstraZeneca’s spinout of Evinova is so interesting – it’s potentially a well-timed move to capitalize on an adoption inflection point for digital biomarkers in biopharma. Still, growth will not occur overnight and not without a clear value proposition and strategy.
Whether you are an R&D leader, a biopharma CEO, a digital health innovator, or a regulator, you need to clearly answer 2 critical questions within your context:
- How can you best think about appropriate (and not) use-cases for digital biomarkers?
- How can you recognize and mitigate key risks to gain buy-in from key stakeholders who have it in their power to decide to use or block digital biomarkers?
For this article, we define digital biomarkers as “quantifiable human data autonomously collected by digital devices.” These devices could include wearables, implanted sensors, smartphone-based sensors, and other monitoring devices.
Value proposition varies by use case
Current trials using digital tools mostly study conditions that can be tracked using a few well-established biomarkers such as glucose levels, heart rhythm, and movement. To expand beyond these, we need to leverage 5 intrinsic and distinct characteristics of digital biomarkers:
- Remote (collecting data where patients live rather than clinical sites)
- Passive (measuring without patient action)
- Natural (gathering data during normal states)
- Continuous (frequent data collection)
- Engaging (creating a positive user experience for patients, caregivers, and clinicians or researchers)
Depending on the context of a specific study, some of these features may be more important than others. To gain acceptance and drive adoption of these tools, digital health leaders must be able to precisely articulate the relevance of each of these characteristics to the specific trial context, and qualitatively or quantitatively identify these benefits. These benefits could include: higher quality data, better context data, improved recruitment and retention, lower cost, and more. Table 1 summarizes select examples of these benefits.
Table 1. Characteristics and benefits of digital biomarkers in clinical trials
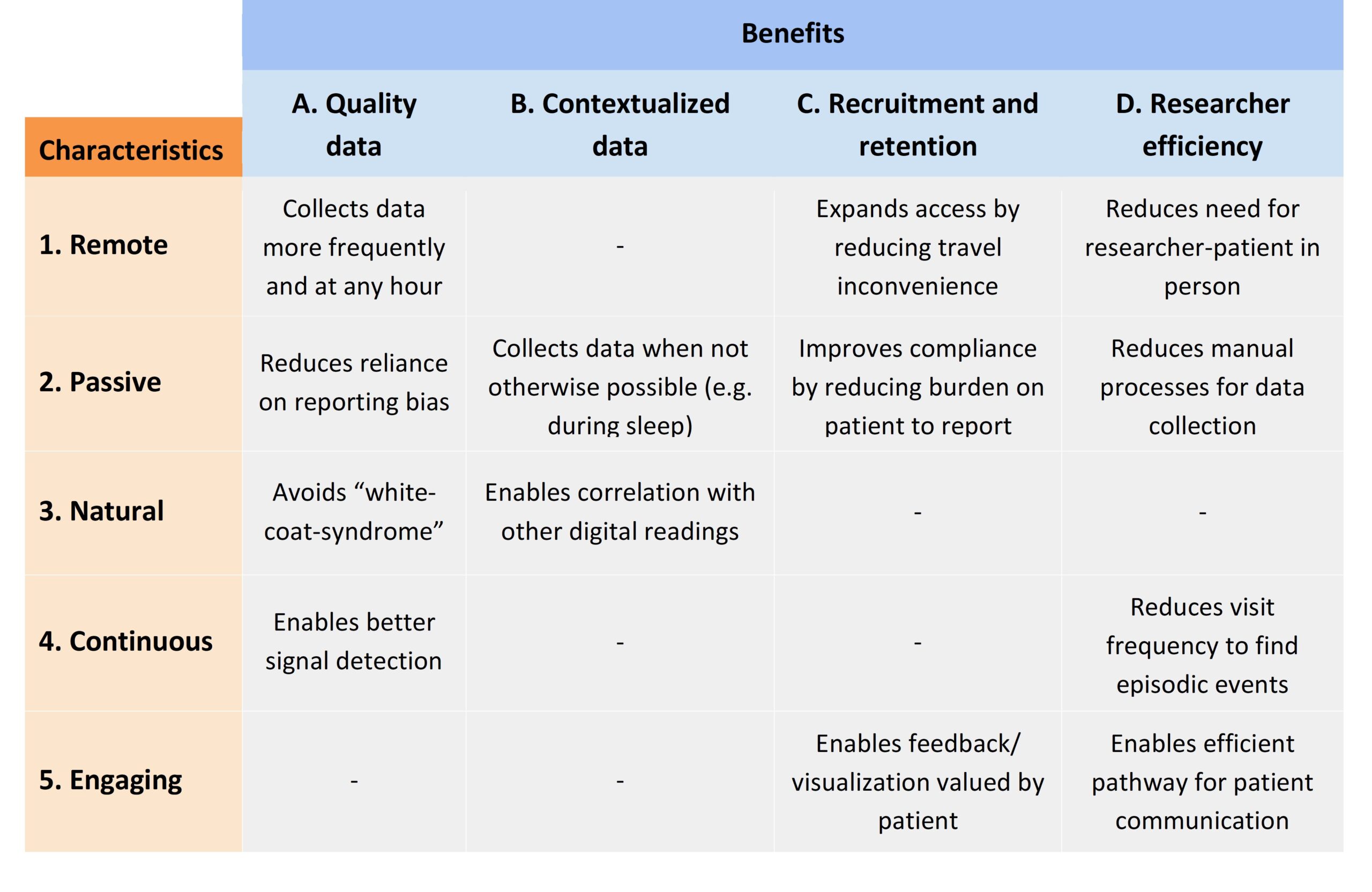
Many studies have leveraged digital biomarkers to enhance both patient care and research efficiency. For example, continuous glucose monitoring (CGM)—available and refined since the late 1990s—improves compliance by automating blood glucose measurements, eliminating the need for patients to perform multiple manual tests daily (C2 in the table above). It also prevents patients from misreporting their glucose measurements (A2), and can trigger automated patients reminders to administer insulin based on digital readings (D5). In addition, researchers benefit from CGM’s continuous data output, which obviates the labor-intensive process of manually logging glucose levels around the clock (D2).
Today, the application of digital biomarkers extends well beyond early tools like Holter monitors and CGM. Wearable sensors are now used to detect subtle gait anomalies, such as early-morning akinesia in Parkinson’s disease, without requiring in-clinic data collection (D1) or patient self-reporting.[1],[2] This also makes trials more accessible to rural patients, and others who do not have easy access to clinical trial sites (C1). Furthermore, these wearable sensors yield high-frequency (A1), passive data that minimizes reporting biases (A2) and reduces fluctuations associated with in-clinic measurements (A3).
The Apple Heart Study (NCT03335800) further illustrates these advantages by continuously collecting high-quality atrial fibrillation data (A4) and directly uploading them in processable formats, allowing researchers to identify fibrillations without any clinical visits (D4). Moreover, continuous monitoring enables the passive collection of contextual data (B2)—such as recognizing naturally lower heart rates during sleep (B3)—to improve the accuracy and meaningfulness of event detection. In addition, user-friendly data visualization on devices like the Apple Watch empowers individuals to monitor and manage their health more effectively, ultimately improving adherence to device usage (C5).
Adoption risks, and steps to mitigate them
A compelling value proposition alone is not sufficient. Even when benefits are clear, digital biomarkers are often not used in a clinical trial due to risk aversion. With already daunting odds associated with bringing drugs to market, investors and R&D leaders understandably hesitate to introduce additional uncertainties. Digital health leaders not only need to demonstrate a clear understanding of the risks but also outline plans to mitigate them. They could also highlight that, in some cases, using a digital biomarker may help reduce overall risk.
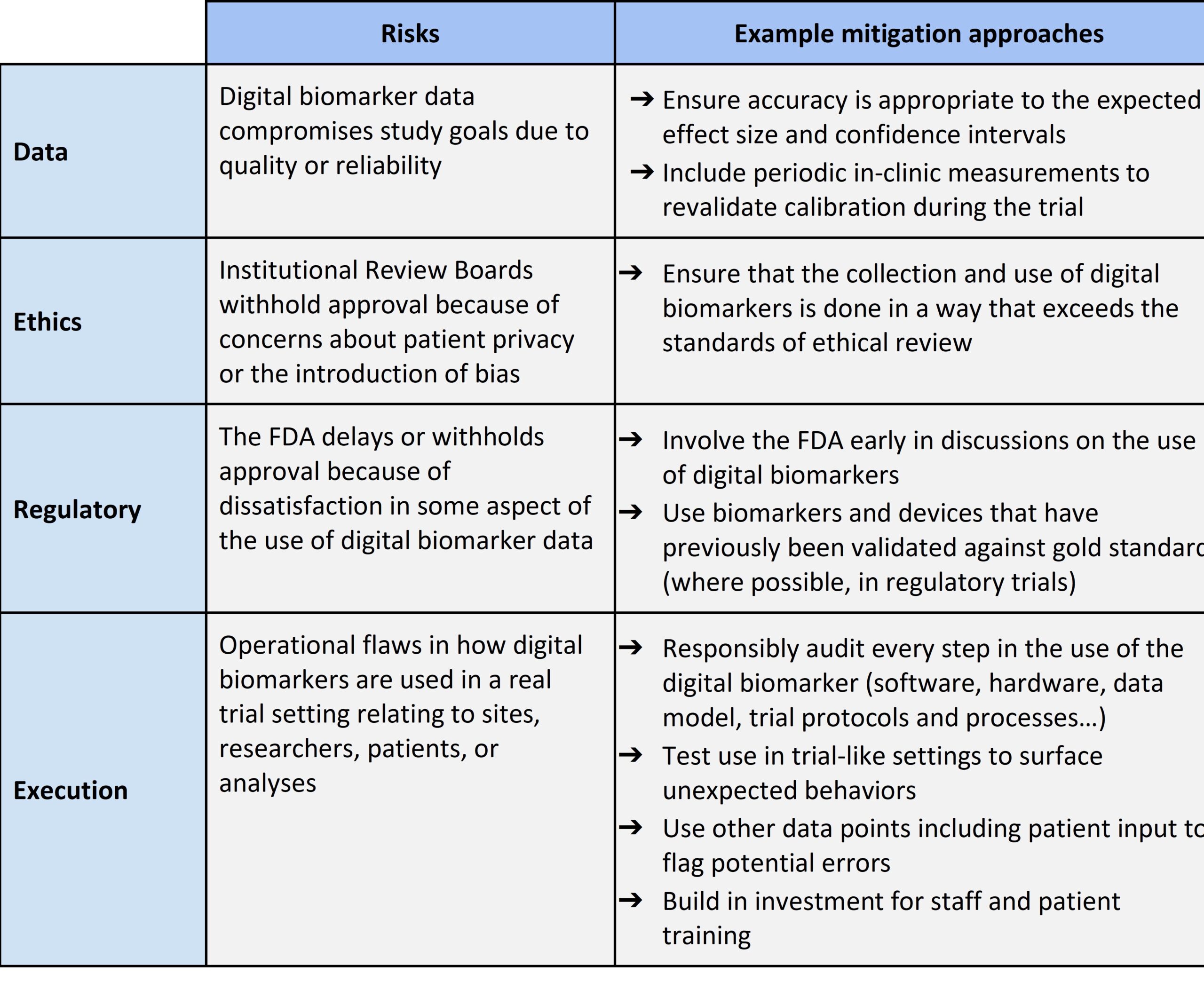
There are 4 interrelated areas of risk we need to consider: Data, Ethics, Regulatory, and Execution. While these areas may overlap, their impact on hesitation to adopt digital biomarkers varies by specific trial context. Table 2 provides a summary of these risks and some example mitigation approaches.
Table 2. Risks of digital biomarkers and example mitigation approaches
Several past clinical trial failures provide valuable lessons about these risks and highlight mitigation strategies that could have improved their success.
Bellerophon Study – a lesson on data quality and privacy
A 2019 Bellerophon phase III trial for fibrotic interstitial lung disease[3] illustrates data risks in digital biomarker implementation. The trial failed partly because researchers did not allow sufficient time for device calibration, failed to plan adequately around handling missing data, and overlooked seasonal and individual behavior variations – undermining its primary outcome measure of time spent in moderate-to-vigorous physical activity. Additionally, the continuous virtual collection of data through digital devices increased patient vulnerability to online attacks. These challenges demonstrate how digital biomarker data can compromise study goals due to quality or security issues.
To mitigate similar risks, researchers can conduct sense-checks on a smaller scale before trial rollout, integrate digital biomarkers with electronic health records to contextualize collected data, incorporate occasional in-clinic visits to validate sensor readings (as demonstrated in a multiple sclerosis trial)[4], and corroborate sensor measurement outliers with patient feedback[5]. Study protocols should also implement multilayer security measures and pressure-test both software and hardware used in studies.
HIV Research – a lesson on ethics
HIV research reveals unique ethical and execution challenges associated with digital health technologies. Clinicians reported that participants downloading secure monitoring apps risked unintentionally disclosing their study involvement to partners or family members – a serious privacy concern.[6] These issues, combined with participation fatigue, shame, and potentially falsified or unreliable data, have contributed to researchers’ reluctance to fully embrace digital health tools to monitor patients.
Firms can address these concerns by ensuring robust security measures such as time-restricted access and multilayered authentication, factoring social pressures into trial design, and developing standardized privacy protocols. Additionally, equipping study coordinators and clinicians with the tools to succeed—through comprehensive staff training, system testing, and standardized privacy protocols—can empower clinical teams to adopt innovative digital health technology to improve both trial efficiency and patient care. By learning from previous failures, future study design can design digital biomarker collection processes that reduce the risk of harm to patients, ensuring they exceed ethical review standards of privacy and safety.
Regulatory lessons – using qualified biomarkers whenever possible
Regulatory guidance suggests that digital tools measuring established biomarkers face a simpler approval pathway than those proposing entirely new surrogate endpoints, which require comprehensive validation of both the measurement tool and the clinical relevance of the endpoint itself.[7],[8] To mitigate regulatory risks, companies should involve the FDA early in discussions, use devices previously validated against gold standards whenever possible, and remain actively engaged with evolving regulatory guidelines.
WEAICOR Study – a lesson on execution and engagement
The WEAICOR study (Wearables to Investigate the Long-Term Cardiovascular and Behavioral Impacts of COVID-19) highlights execution and patient engagement challenges in digital biomarker trials. Researchers encountered significant compliance issues affecting adherence to wearing the Biostrap device.[9] While overall compliance decreased as the study went on, younger patients and those with less severe disease were less compliant than average. External environmental factors (Hurricane Ida occurred during the overall study period, and there was a dramatic decline in compliance) also contributed to patient non-compliance. Similar issues affected other studies: in one study involving heart failure patients, adherence to smart pill bottle usage was particularly low, with 55% of participants using them less than 10% of days.[10] Studies of Parkinson’s and Huntington’s disease patients also saw compliance to smartphone apps, smartwatch streaming, and structured motor task participation drop 34-53% over 6 months.[11]
However, these patient engagement and execution risks can be addressed through real-time compliance monitoring systems. Trial designers can create automated alerts to track adherence and trigger tiered interventions, such as reminder texts, phone calls, or investigator outreach, when devices remain idle. Researchers can collect post-trial participant feedback to understand root causes of non-compliance, and refine future strategies accordingly. Insights from existing remote trials suggest several effective approaches to improve patient engagement: minimizing daily survey burdens, offering meaningful incentives to sustain participation, and incorporating periodic in-clinic visits as engagement checkpoints. By adopting these strategies, digital health teams can improve compliance and ensure more reliable trial outcomes.
Conclusion
Digital biomarkers are no longer just a pipe dream—they are here, and their use is potentially at an inflection point. However, successful implementation requires more than enthusiasm; it demands thoughtful strategies tailored to each clinical innovation, therapeutic area, and digital tool.
For executives weighing whether to adopt these transformative technologies, the question is not “if”, but “how.” The stakes are too high to wait on the sidelines. Whether you’re leading R&D, digital health, or overseeing operations, this is the moment to take a closer look at how digital biomarkers can accelerate your organization’s goals.
–
[1] Poplawska-Domaszewicz K, et al. Parkinson’s Kinetigraph for Wearable Sensor Detection of Clinically Unrecognized Early-Morning Akinesia in Parkinson’s Disease: A Case Report-Based Observation. Sensors (Basel). 2024;24(10):3045. Published 2024 May 11. doi:10.3390/s24103045
[2] Moreau, C., Rouaud, T., Grabli, D. et al. Overview on wearable sensors for the management of Parkinson’s disease. npj Parkinsons Dis. 9, 153 (2023). https://doi.org/10.1038/s41531-023-00585-y
[3] Tackney, M. S., et al. (2024). Unleashing the full potential of digital outcome measures in clinical trials: eight questions that need attention. BMC Medicine, 22(1). https://doi.org/10.1186/s12916-024-03590-x
[4] Daniore, P., et al. (2024). From wearable sensor data to digital biomarker development: ten lessons learned and a framework proposal. npj Digit. Med. 7, 161 https://doi.org/10.1038/s41746-024-01151-3
[5] Eagleson, R., et al. (2017). Implementation of clinical research trials using web-based and mobile devices: challenges and solutions. BMC Medical Research Methodology, 17(1). https://doi.org/10.1186/s12874-017-0324-6
[6] Andriesen, J., et al. (2017). Using Digital Technologies in Clinical HIV Research: Real-World applications and Considerations for Future work. Journal of Medical Internet Research, 19(7), e274. https://doi.org/10.2196/jmir.7513
[7] https://www.fda.gov/drugs/biomarker-qualification-program/pathways-biomarker-integration-drug-development#language
[8] https://www.fda.gov/drugs/biomarker-qualification-program/qualifying-biomarker-through-biomarker-qualification-program#1
[9] Mekhael, M., et al. (2023). Compliance challenges in a longitudinal COVID-19 cohort using Wearables for continuous Monitoring: observational study. Journal of Medical Internet Research, 25, e43134. https://doi.org/10.2196/43134
[10] Sohn, A., et al. (2020). Integrating remote monitoring into heart failure patients’ care regimen: A pilot study. PLoS ONE, 15(11), e0242210. https://doi.org/10.1371/journal.pone.0242210
[11] Cohen, S., et al. (2018). Characterizing patient compliance over six months in remote digital trials of Parkinson’s and Huntington disease. BMC Medical Informatics and Decision Making, 18(1). https://doi.org/10.1186/s12911-018-0714-7