
A clinical vignette: the cases of Jane and Joe
Imagine if you will two individuals both at age 50. Jane is a project manager whose recent health care has focused on managing menopausal symptoms, a knee injury sustained while skiing, and moderate episodic depression, with a medication list of one chronic medication, and one medication as needed. Joe is a bus driver whose recent health care has focused on managing Type II diabetes, hypertension, and low back pain, with a regimen of 4 chronic medications, and 2 medications as needed. Jane is highly informed and engaged in her care. Joe is also engaged, but less informed, and is facing a more difficult home and personal finance environment.
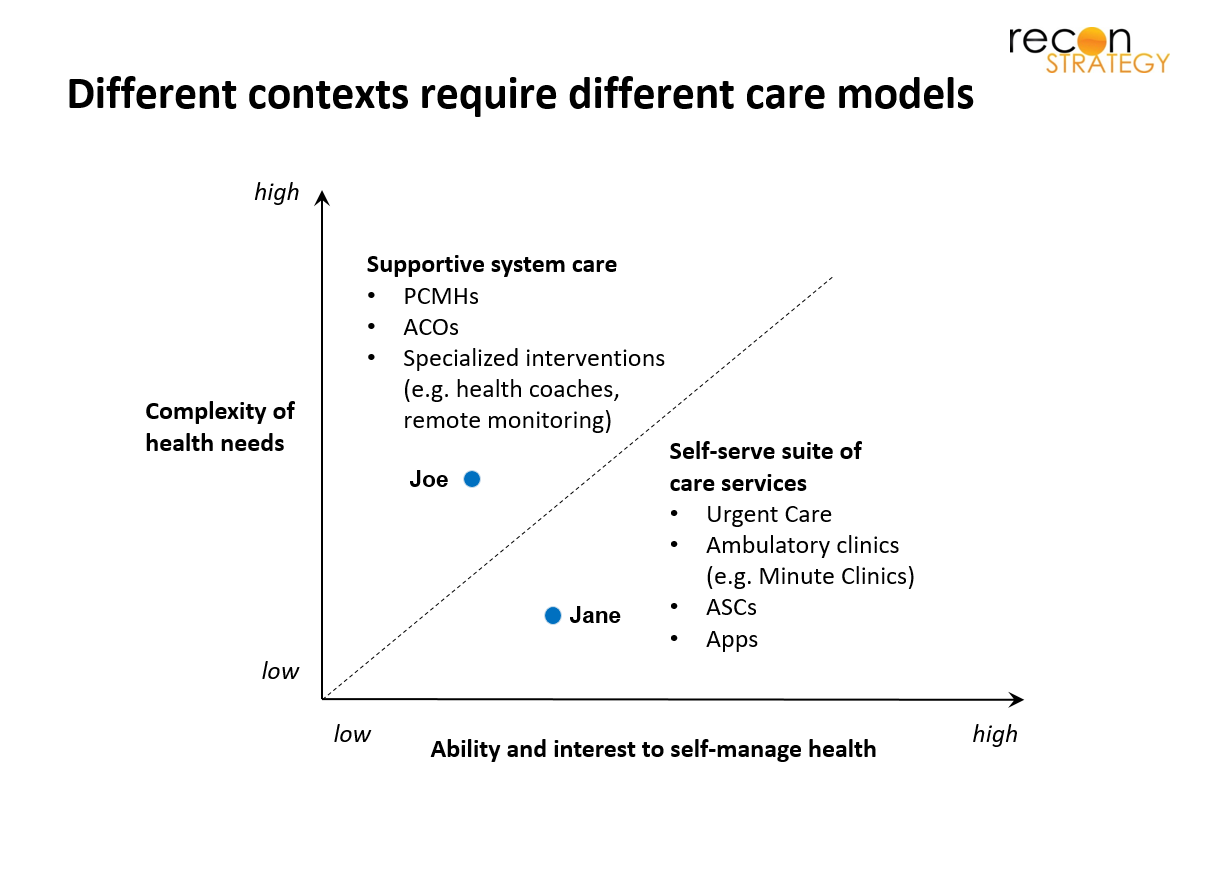
The crux of the question we’d like to pose is whether Jane and Joe will be best served by receiving care through modulation of a single common delivery model, or whether at this stage of their specific respective circumstances, they should be receiving care under delivery models that are different.
Our hypothesis is that given recent trends in specialization of care as well as in consumer-oriented technology there is a need (or opportunity) for differentiated care models that fall into two main categories: one based on a supportive system of care (for example a Patient Centered Medical Home (PCMH)), and the other based on a self-serve suite of care services (for example Urgent Care (UC)). Two key segmentation variables drive this differentiation: (1) the complexity of health needs, (2) the ability and interest to self-manage health.
In this brief working paper, we sketch a picture of recent drivers that support a bifurcation of models of care, as well as inefficiencies that arise when the wrong care model is applied to a given population. Finally, we speculate on factors that will drive success in this new environment.
Trends in models of care: an evolving tug of war between professionally managed care and self-directed care
Looking back a generation, one can already identify two driving forces which is in some sense were pushing care models in opposite direction. Back then, a paternalistic physician corps ran the show while payers were largely customer aggregators and payment processors. Fast forward 30-40 years, physicians have become much more transactional while payers are getting involved in care management and pushing value (or at least trying to).
However, right now, the most important driver of change is neither provider-centric nor payer-centric. It is the fact that technology is gradually empowering many members/patients to become consumers capable of self-directed care – and this in a variety of ways:
- Access to medical knowledge: It seems hard to believe that just 20 years ago, it was hard for a patient to access medical information – first because it was located in books tucked away in medical libraries, and second because the books were written in a language inaccessible to lay persons. Today, medical information is readily available in a way that is much more digestible, and for example typing one’s symptoms such as “excruciating flank pain” into a search engine immediately suggests a diagnosis and an avenue for confirmation and treatment.
- Access to one’s medical record: Before digitization, medical records lived in unwieldly thick files and one had to beg and plead (and sometime pay) to get hard-to-read photocopies which mixed the irrelevantly trivial with critical information in a mess of paperwork. EMRs and claims databases coupled with patient/member portals have not solved all that, but they are a giant leap forward, enabling an engaged patient to make direct use of their data in care decisions.
- Access to modular options for care: The last element that technology is providing to members/patients is information and access to a menu of care services – ranging from finding out which Urgent Care center is nearby, to accessing telehealth options from anywhere, to ordering one’s own labs, to doing price comparisons between various service offerings.
For some individuals, these innovations are clearly making a big difference in how they access health care, but across a population, there are large segments that still rely on a more classical model professionally managed care and will continue to do so. For example, it may well be beyond the ability of a patient faced with a complex and/or debilitating condition to engage with those types of tools when they are already struggling in day to day life activities.
Properly sorting members/patients into a self-directed care model or a managed supportive care model is important, but not so easy
Managed supportive care is expensive because it requires paid staff to take real responsibility for patient needs – to be in the clutch role such that when “something” (which could be a nebulizer for the home, an appointment with an ENT, a third follow-up on a radiology study that showed something suspicious, etc.) is needed, that need will be covered regardless of the number of phone calls or complexities that must be overcome. It can create significant value, in terms of health, and sometimes savings, but only for specific populations – for instance, PCMH-type initiatives have shown limited impact when applied to broad panels of patients.
On the other hand, a self-directed care model can also be expensive, and worse, lead to poor outcomes. It can lead to skipping preventive care with dire consequences down the line, or seeking care in the wrong setting (e.g. ED instead of UC, sub-specialist where an NP would have been adequate etc.). But often, removing a processing layer, and placing the burden of chasing loose ends of care on the member/patient rather than on a third party can save significant cost and be more effective than doing the same via a bureaucracy. In addition to these considerations, the fact remains that a significant segment of the population is interested in self-directed care, and that in a competitive market, some players will focus on serving that interest unless regulation forbids it.
Playing in both worlds is challenging for a provider organization, because when a provider builds the culture to go the extra-mile for a set of patients, it is hard for that same organization to simultaneously take an approach to be hands off for another set of patients.
A few success factors in the new world of bimodal care
Assuming for now that the split of care models will occur, what are the characteristics and capabilities that will optimize care delivery? We list the four that we deem the most important.
The first is obviously the ability to sort or steer members/patients into the appropriate model of care. Core to this is a question of tailored information, advice and incentives which are not easy to get right, for the patients, for the providers, and for the payers.
Second is that members that go the self-service route would still benefit from a type of light support. They are willing to do their homework and research care options, but in some instances will be well served by clarifications that a knowledgeable expert can provide quickly. Someday AIs will do that, but until then a service that supports and empowers individuals who need 10 min of expert consultation could make a huge difference.
Third, for those patients who need full-service organization of their care, an orchestrator of care who is able to seamlessly plug otherwise self-serve modular services (e.g. free standing imaging, ASCs or UCs) into their system of care will be advantaged because that means an ability to shop for quality and price rather than relying on a static referral destination. United/Optum appear to be working hard to develop that capability.
Fourth and finally, service lines which set themselves up as dually capable of serving both population – either through classic referral pathways, or through self-service will win. This level of ambidexterity, i.e. being part of a “system” and at the same time open to the marketplace is not something that is easy to join under one roof, but multiple organizations have managed this successfully (e.g AMZN) so not impossible to achieve in healthcare as well.
So what does this mean for Jane and Joe?
Recall Jane our well-off, well-informed project manager with minor health issues, and Joe, our struggling bus driver with hypertension, diabetes, and low back pain.
- For Jane and Joe, the phenotype of the PCP that will provide the best value[1] is totally different. For Jane it is a PCP who is efficient with time and quick to delegate responsibility to Jane. For Joe it is a PCP and a care management team that will go the extra mile for instance following-up proactively to understand what is happening when Joe fails to fill a prescription.
- If Jane is going to be manage her health semi-autonomously, she could greatly benefit from on-demand expert advice through a help-line for instance “I have been having symptom X, can I expect this to resolve, and how long should I reasonably wait before seeking an evaluation – and where?”
- Even though Joe needs substantial wrap-around care, Joe should still be able to access highly efficient, assembly line like components of care, for instance a screening colonoscopy at a high-volume ASC. That implies that Joe’s care team is able to efficiently communicate with such sites and ensure that there is excellent follow-up.
- Conversely, a high-volume ASC should be able to provide its services to Jane and Joe in a way that establishes information flow at the appropriate level – making the information usable by Jane herself, but also by Joe’s care team.
[1] In the Michael Porter sense, health benefit divided by cost