
Iora Health was one of the original primary care transformers offering a clinically capable, engagement-focused, and accountability-grounded care model. After an initial foray into commercial, Iora pivoted in 2014 to Medicare Advantage (MA), an alliance with HUM and a global capitation-oriented strategy broadly similar to Oak Street or ChenMed.
MA – whose members often have chronic conditions that respond to management and with a payment model that rewards quality (via stars) and patient intimacy (via risk coding) – is fertile ground for Iora’s high touch primary care. And that terrain is wide open. The patient panels of these players are typically measured in tens of thousands while MA has 26M members and is growing fast. Iora raised another $126M in early last year which should theoretically have helped it push hard into the patient landgrab.
A bare 18 months after raising the money, Iora has sold itself to ONEM, an entirely different type of primary care organization. ONEM offers premium concierge, membership-based care experience for the commercial market. It also has economics curiously dependent on big payments from integrated delivery systems (under the frame of “strategic alliances”). The purchase price put Iora’s per-patient valuation at 45% that of Oak Street[1]. Legacy Iora now makes up more than 25% of the market value of the combined entity. The Iora deal is expanding ONEM’s TAM from $170B (commercial) to $870B (MA and direct contracting) per analysts. Yet, only one top executive from Iora will remain and that as Chief Innovation Officer, a role usually well removed from strategic and operational influence.
What happened?
Inability to control medical costs
Iora is struggling to manage care costs. On a per-patient basis, Iora reports both higher external (referral care, facilities, Rx, etc.) and internal care costs (primary care providers, patient support team and the clinics) compared with Oak Street.
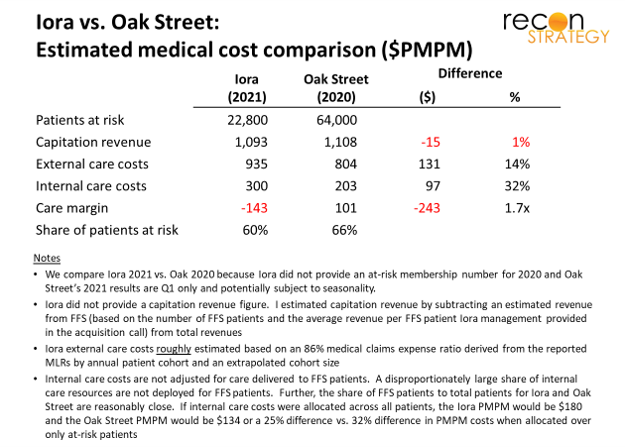
Note: Iora’s lower overall operating scale (35% as many patients at risk as Oak Street) may be part of the issue, although market density and clinic-level scale is usually more important for managing care (see below). Operating scale plays a larger role in administrative overhead not included in the economic comparison above.
Iora’s model is differentially focused on health coaches working closely with patients. In our experience, coaches can do wonders with behavioral and SDoH challenges. However, the clinically complex issues common among Medicare eligibles may be more resistant to coaching-focused engagement.
Struggling to grow
Poor medical cost performance in any one year might be a function of rapid growth: high touch primary care can need years to whittle away at previously untended issues of its patients. And, certainly, Iora was investing in growth over the last couple years:
- Opening new markets in Houston, Georgia, and North Carolina
- Expanding its relationship with Humana in Georgia, Texas, and Arizona in 2019
- Signing new contracts in 2021 with Aetna (Houston), Devoted Health (Phoenix and Houston), and Cigna (across its national membership).
Results, however, seem disappointing. Iora expects 40% revenue growth between 2020 and 2021 (estimated). Back when Oak was about the same scale as Iora (in 2018), it grew revenues 75% in the subsequent year (and grew patients 62%) and still improved its care margin from 1% to 5% year over year. Even in 2021, at more that twice the patient scale, Oak is expected to grow revenues by 50%. More ominously, the competition – with the active support of Iora’s old strategic partner HUM – is increasingly active in Iora’s markets, constraining future growth:
- Oak Street has announced plans to launch in Arizona
- Partners in Primary Care (a HUM joint venture) and VillageMD are heavily investing in growth in Houston
- Heal is launching in North Carolina and Washington (as well as other markets) backed by $100M investment from HUM
Fragmented footprint locking in cost disadvantage
Local market density is critical for advanced primary care. If you have threshold scale, you can more easily persuade referral and facilities partners to collaborate with your care management protocols. You can also structure the care teams in each location more efficiently. Iora appears to have scattered itself too thinly in its quest for growth.
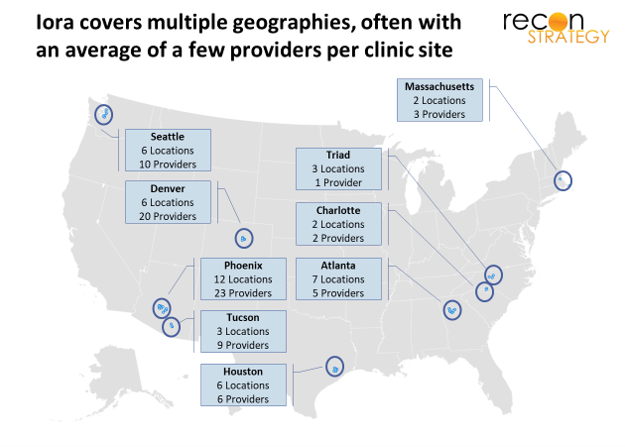
Iora has just 32 providers in its Phoenix/Tucson flagship (out of a total of 80[2]) while Oak Street has ~150 providers in its flagship greater Chicago market (out of a total of 265). Across their respective clinic footprints, Oak Street has about 2x the number of providers per location vs. Iora. Oak Street’s larger per clinic team enables more clinical leverage: about 50% of Oak Street providers are mid-levels vs. 10-15% for Iora. Of course, Iora’s lower share of APPs could be by design with coaches being the primary source of leverage for physicians. However, small clinic sizes will also make it harder for Iora to shift its model to increase clinical leverage.
Instability in the talent
For advanced primary care, provider retention is critical for several reasons:
- Patient trust with their provider is key to outcomes but takes time to build
- The right clinical phenotype is rare and being aggressively recruited by many
- Having enough veterans on the team can more quickly integrate new providers into a practice’s protocols and culture.
Yet, on the retention dimension, too, Iora seems to be struggling[3]. Iora and Oak Street both recruited a lot of providers in the past year. However, Iora also saw a much larger share of departures in the same period: Per Physician Compare, 40% of Iora’s providers in late 2019 were no longer employed at Iora by early 2021 while only 20% of Oak Street’s providers departed over the same period.
Iora has also seen significant turnover in leadership: of the 8 top executives, 2 (the CFO and CGO) joined just a few months ago, and two others (the COO and the CMO) joined in 2019. Prior to these changes, Iora’s leadership was stable and largely promoted from within: the former CFO had been with Iora for 6 years, the former Chief Product Officer for 9 years, the former EVP for Market Operations for 6 years and the former Chief Growth Officer for 4 years, rotating through tenures via multiple promotions.
* * *
For high touch primary care, MA global capitation offers many levers for success: opportunity to deeply engage patients crying out for clinical management, large rewards for improving quality and patient experience, big revenue lift for getting the diagnostic coding and documentation right. Yet having the right idea and being in the right market is not enough. Iora did not figure out how to convert engagement into care margin, found its growth opportunities blocked and struggled to hold on to talent. No wonder Iora decided to sell.
Iora’s takeover by ONEM has been broadly praised by analysts: ONEM now has contracts with MA, a pathway to hold on to its commercial members as they age into Medicare, and a story about operating synergies and combining the best from each of the technology platforms. It is unclear how much of legacy Iora will be left as more of the talent cashes out.
Iora was widely respected as a highly innovative, mission oriented, savvy provider group which opened a lot of eyes to what primary care could be. This conclusion to the Iora tale is perhaps one more example of the old business strategy adage that innovators struggle to capture the rewards themselves but rather end up pointing the way to big winnings for fast followers.
[1] Measured as market capitalization divided by at risk members. For Iora, I used the 2021 figures and acquisition price. For Oak, I used the Q1-2021 membership and last week’s market capitalization.
[2] Per datasets in Definitive Healthcare.
[3] Using Physician Compare in this way requires some caveats as the data is not always updated in a consistently timely way. For example, for the latest Physician Compare data set, Oak Street has 164 primary care providers while Definitive Healthcare’s data set has 265. These figures must be taken as rough indicators of a moving target. Calculation includes only MDs in primary care specializations and APPs. Not included were ancillary clinicians (e.g., physical therapists, social workers) or physicians with other non-primary care specializations (e.g., psychiatry).